Director of the Stem Cell and Retinal Regeneration Program at the Gavin Herbert Eye Institute (GHEI), Henry Klassen, MD, Ph.D., leads life-changing research that will affect and influence vision-saving treatments for years to come.
Watch below to hear from Dr. Klassen on his recent stem cell research:


 When you think of cancer, most of us do not think about the eye or vision. Though rare, cancer can start inside or outside of the eye. If cancer starts inside the eyeball it’s called intraocular and if it starts outside the eye (eyelid or in the eye socket) then it’s called extraocular tumor. It can occur in both children and adults. Most major eye centers have specialists who are trained in the diagnosis and treatment of eye cancers.
When you think of cancer, most of us do not think about the eye or vision. Though rare, cancer can start inside or outside of the eye. If cancer starts inside the eyeball it’s called intraocular and if it starts outside the eye (eyelid or in the eye socket) then it’s called extraocular tumor. It can occur in both children and adults. Most major eye centers have specialists who are trained in the diagnosis and treatment of eye cancers.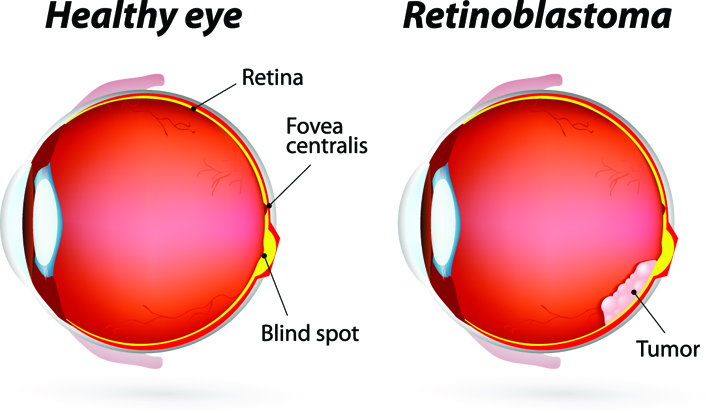 At the later stage of this cancer, the only one way to survive is to remove the eyeball (enucleation). Like many of other types of cancer, retinoblastoma has a genetic component so genetic testing needs to be done. The tumor begins with the RB1 gene mutation that stimulates retinal cells to develop into a tumor called a retinoblastoma. The RB1 mutation can be inherited from the parents, but in some cases it is sporadic and not inherited. There are various treatments such as surgery, chemotherapy, radiotherapy etc. to cure retinoblastoma cancer. Rarely it can spread beyond the eye.
At the later stage of this cancer, the only one way to survive is to remove the eyeball (enucleation). Like many of other types of cancer, retinoblastoma has a genetic component so genetic testing needs to be done. The tumor begins with the RB1 gene mutation that stimulates retinal cells to develop into a tumor called a retinoblastoma. The RB1 mutation can be inherited from the parents, but in some cases it is sporadic and not inherited. There are various treatments such as surgery, chemotherapy, radiotherapy etc. to cure retinoblastoma cancer. Rarely it can spread beyond the eye. 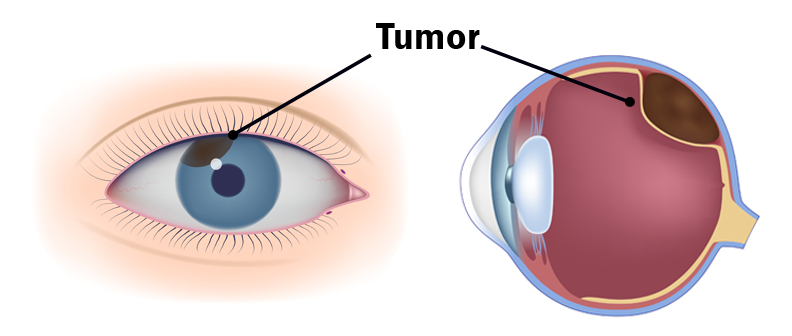
 Tom Sullivan
Tom Sullivan

 Lauren Hauptman
Lauren Hauptman
 Tom Sullivan
Tom Sullivan