
 Best wishes to you and your family this Thanksgiving. We will continue posting the articles you enjoy on Tuesday December 2nd, which is also #GivingTuesday. If you have liked our posts and found them useful, please consider a donation to the Discovery Eye Foundation.
Best wishes to you and your family this Thanksgiving. We will continue posting the articles you enjoy on Tuesday December 2nd, which is also #GivingTuesday. If you have liked our posts and found them useful, please consider a donation to the Discovery Eye Foundation.


Adjustments Can Help With Depression
11/25/14
Eye disease can lead to isolation and depression. But making some adjustments can help with the depression. Robin Heinz Bratslavsky (pictured below with her oldest son) was diagnosed with keratoconus (KC) 20 years ago at age 25. Now a mother of two who works from home as a freelance editor. She participates in NKCF’s KC-Link.

When I was diagnosed with KC, I was an editor at a major women’s magazine. The diagnosis didn’t mean much to me at the time. Things changed when I was fitted with RGPs. I had limited wear time and pain, and I started to feel anxious about my career. There were times I had to leave work early and drive to my eye specialist — several times a week. As a young editor in a highly competitive field, I was concerned these absences would interfere with my ability to move up at the magazine.
When I had my first child, my husband and I decided I would stay home with him and work on a freelance basis. I’ve been doing this for 14 years now. Through a series of corneal abrasions, infections and lens-tolerance issues, I have had to rely heavily on my husband and family and friends to drive me and my children when my eyes would not cooperate. I have had moments of extreme despair, because I am not used to being so dependent. My husband works incredibly long hours, and he used to travel a lot. I was always worried I would not be able to drive my children in an emergency.
As my KC has progressed, I have moments in which my normally well-controlled clinical depression manifests, and I feel helpless because of my vision limitations. My sons are both avid soccer players, and I miss a lot of their on-field accomplishments, because I simply cannot see well enough.
At this point, I wear Kerasoft lenses, and I have had Intacs placed in my right eye. My vision, corrected, is about 20/30, but that can vary from day to day. After 20 years, it appears my KC is stabilizing, so I have a pair of emergency glasses; they get me to approximately 20/60, so I can’t drive, but I can function somewhat around my house to give my eyes a break. I’ve been living with KC for a long time; it’s a manageable disease — as long as you are willing to make some adjustments.
 Robin Heinz Bratslavsky
Robin Heinz Bratslavsky
Keratoconus Advocate
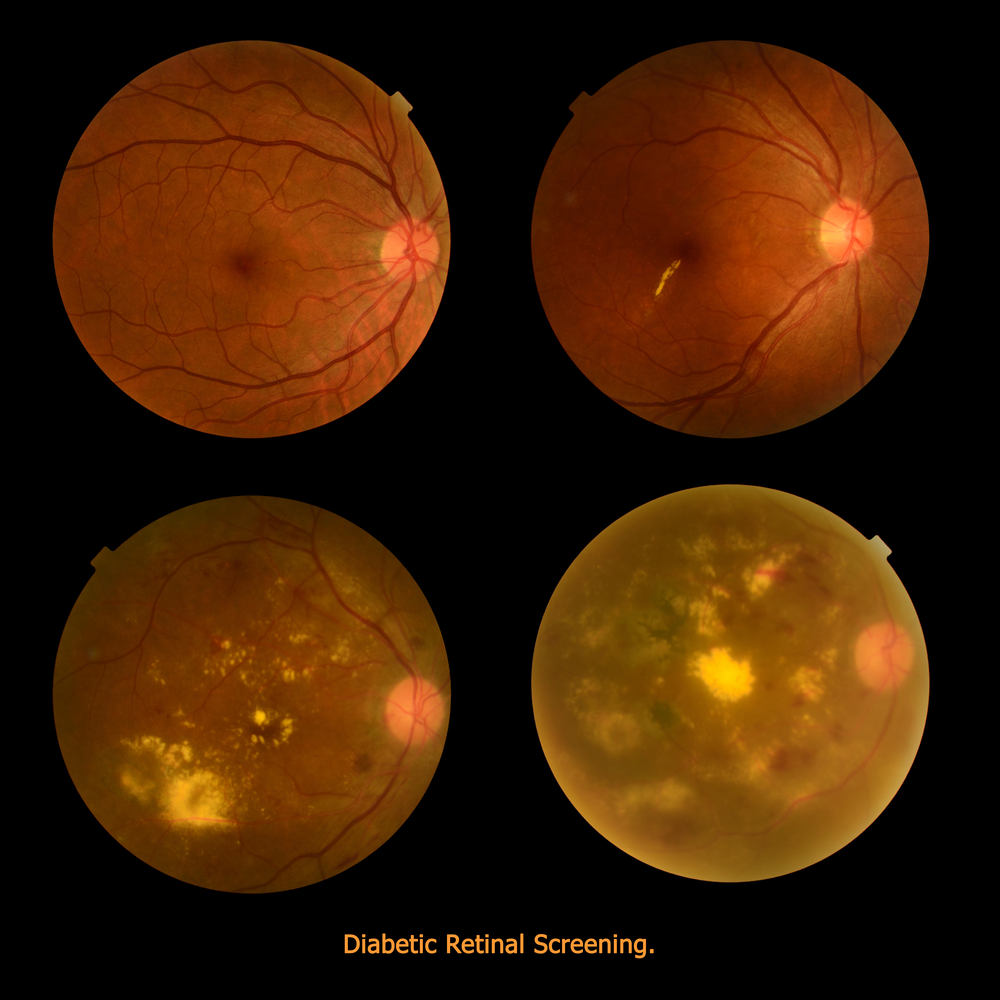
Diabetes And The Potential For Diabetic Retinopathy
11/20/14
Defining Diabetes
Diabetes mellitus is a group of metabolic disorders in which a person has high blood sugar levels. It occurs either because the pancreas does not produce enough insulin, or because the body does not respond appropriately to the insulin that is produced. Insulin is the hormone that converts sugar into energy for the body. There are several forms of diabetes.
Type 1 diabetes occurs when the pancreas does not produce adequate levels of insulin. It usually develops during childhood or adolescence; however, it can also occur in adults. Those with type 1 diabetes must take insulin injections. About 10 percent of those with diabetes have type 1.
Type 2 diabetes is the most common type of diabetes, affecting about 90 percent of those with diabetes. It is caused by the combination of the body’s resistance to insulin (not using its own insulin efficiently) and the pancreas not producing enough insulin. As a result, there is an increase in the level of sugar, or glucose, in the blood.
Gestational diabetes occurs in pregnant woman who have not previously had diabetes but whose blood sugars become elevated during pregnancy. In many patients, their blood sugars will return to normal after the pregnancy is over. Placental hormones make the mother resistant to insulin, causing a buildup of blood sugars. These women are at high risk for type 2 diabetes later on in their lives.
Diabetic Retinopathy: An Overview
Anyone with uncontrolled diabetes is at risk for developing diabetic retinopathy. According to the National Eye Institute, between 40 to 45 percent of Americans with diabetes have some form of diabetic retinopathy, the most common eye condition associated with diabetes.
In the United States, the Centers for Disease Control and Prevention reports between 12,000 and 24,000 new cases of blindness each year due to diabetic retinopathy, making it the leading cause of vision loss among American adults, ages twenty to seventy-four. The Center also projects that by 2050, the number of Americans age forty and older with diabetic retinopathy will grow from a current 5 million individuals to about 16 million. Although these statistics are alarming, you can prevent or delay damage to your vision by controlling your diabetes, along with obtaining regular eye evaluations and treatment.
Defining Diabetic Retinopathy
Diabetic retinopathy is a disease affecting the retina, caused by elevated blood sugar levels. It usually affects both eyes and occurs when uncontrolled blood sugar levels damage the small vessels of the retina, the light-sensitive tissue in the back of your eye. The retina is responsible for processing images that make vision possible. To produce clear, distortion-free vision, the retina must lie completely flat. If the delicate retinal tissue is damaged, images that you see may be blurred or distorted.
Diabetic retinopathy is a progressive disease, and thus worsens over time. Although some effects, such as blurriness and distortions, may be mild or subtle, the long-term consequences can cause severe vision loss.
Symptoms of Diabetic Retinopathy
Because diabetic retinopathy rarely causes pain, symptoms are not always apparent in the earliest stages. In fact, damage to your retina could be occurring long before you have noticeable signs. When symptoms do occur, they’re often caused by retinopathy affecting the macula, the area at the center of the retina. Symptoms may include the following:
• blurred vision
• seeing dark spots or “floaters” (small specs in your field of vision)
• decreased night vision
• vision loss
• problems seeing colors
It’s important that you see your eye specialist immediately if you have any such symptoms. Diabetic retinopathy cannot be cured, but with careful monitoring, it can be diagnosed and treated, before your vision is impaired. The treatment is typically less invasive and more effective when diagnosed at an earlier stage, before permanent damage has occurred.
How the Retina Works
The retina is made up of specialized nerve tissue that contain microscopic receptors (called cones and rods) and other nerve cells that line the back of the eyeball.
These cells carry signals (images that we see) along the optic nerve to a special area of the brain, where they’re interpreted into what we perceive as sight. You might compare the retina to film in a camera—the film delivers the photo image that the camera captures.
There are two main areas of the retina that can be damaged by diabetic retinopathy:
• The macula, the center of the retina. The macula allows you to read and see fine details and recognize colors. At the very center of the macula is a dimple known as the fovea. It is the most sensitive portion of the macula and makes sharp vision possible.
• The peripheral retina, which is the portion of the retina that is outside the macula. It’s responsible for your side vision and also makes night vision possible.
The retina lies on a nutrient-rich flat “carpet” of vessels that nourish it with necessary oxygen and nutrients. To reach the retina, however, nutrients must pass through two buffers—a thin membrane called Bruch’s membrane and a single layer of specialized cells called the retinal pigment epithelium. Waste products are also transported away from the retina through these two membranes. Diabetic retinopathy can interfere with this constant import of necessary nutrients and export of waste products.
Risk Factors for Diabetic Retinopathy
There are many factors that can raise your risk for diabetic retinopathy. However, you’ll note that many of these risk factors can be controlled.
Duration of Diabetes and Glucose Control
The longer you’ve had poorly controlled blood glucose levels, the higher your risk for diabetic retinopathy. Most diabetic individuals develop eye problems overtime, making duration of their diabetes one of the strongest predictors that they will develop this eye disease. Research has shown that nearly all type 1 diabetics and 60 percent of type 2 diabetics develop the condition within the first two decades of their diabetes diagnosis.
The American Diabetes Association (ADA) recommends fasting glucose levels between 70 and 120 mg/dL and less than 180 mg/dL two hours after meals. They also recommend a hemoglobin A1c of 7 percent of less. Hemoglobin A1c is a protein in red blood cells that bonds with blood sugars. Since red blood cells can live from 90 to 120 days, the hemoglobin A1c stays in the blood for that length of time. Accordingly, it is effective in measuring the average blood sugars over a period of time. This test tells doctors how well your treatment plan is working. You should always know what your hemoglobin A1c values are, as they may affect the interval between your retinal examinations.
Obesity
The more fatty tissue you have, the more resistant your cells are to insulin. Obesity increases your risk for diabetes as well as other serious conditions such as heart disease. Estimates suggest that 65 percent of Americans may be overweight. Being overweight aggravates high blood pressure and cholesterol. Achieving a healthy weight is important in controlling blood sugars and diabetes related complications.
Lifestyle Choices
A sedentary lifestyle, especially if you are overweight, contributes to many diseases, including diabetes, heart disease, high blood pressure, and high cholesterol levels. On the other hand, physical exercise improves circulation, lowers blood sugars, and improves your body’s use of insulin. This results in improved blood sugar levels. This benefit of increased sensitivity to insulin continues for hours after you stop exercising.
Exercise also promotes weight loss. A sedentary lifestyle contributes to insulin resistance, and makes it more difficult to keep weight off. Even light or moderate physical activity can help lower blood sugars.
Smoking is another major risk factor for developing diabetic retinopathy. Smoking also causes diabetic retinopathy to progress faster. The nicotine in tobacco not only contributes to higher blood pressure and higher cholesterol levels, but it also impairs insulin activity. Even though quitting can be difficult, it is critical to heart health and diabetes control.
Unlike smoking, alcohol consumption doesn’t have a direct influence on diabetic retinopathy. Yet because it can affect diabetes control, drinking in excess can affect the health of your eyes. Your doctor can tell you what constitutes drinking in moderation for you.
High Cholesterol Levels
Diabetes puts you at risk for chronically high cholesterol or blood fats that promote the buildup of plaque in your arteries. Although the tiniest vessels of the retina are too small for such build-up, uncontrolled cholesterol can contribute to macular edema and the development of hard exudates, the small yellow spots or lipid deposits that may form in the macula. Both conditions are associated with a higher risk of vision loss.
Doctors advise keeping “bad” or low density cholesterol (LDLs) less than 70 mg/dL. Good cholesterol or high density lipoproteins (HDLs) should be greater than 40 mg/dL in men and 50 mg/dL in women. Both men and women should strive for triglycerides, another type of fat, at levels less than 150.
High Blood Pressure
If you have both diabetes and high blood pressure (also called hypertension), you may be at higher risk for a number of eye-related problems, including retinopathy, glaucoma and optic nerve damage. Seriously elevated blood pressure not only stresses your heart, it also raises the risk for eye problems, particularly macular edema and bleeding. Chronic hypertension combined with long-term diabetes also increases the chance that your retinopathy will be more destructive and progress more rapidly. Research has consistently shown that keeping your blood pressure below 130/80 mmHg is important in minimizing the risk of hypertension related complications.
Race/Ethnicity
Diabetic retinopathy is more common in some ethnic and racial groups than others. African Americans, Asian Americans, Hispanic/Latino Americans, American Indians and Alaskan Natives are at higher risk for type 2 diabetes than non-Hispanic whites.
African Americans and Mexicans are almost twice as likely as whites to have eye problems, according to the American Diabetes Association. Native Americans also have an increased for diabetic retinopathy. Researchers aren’t sure why some ethnic groups have higher rates of diabetes, which increase the risk for retinopathy and other problems.
Age and Gender
As mentioned earlier, the longer you have diabetes, the greater your risk for diabetic retinopathy. Not surprisingly, this complication is rare among children but common among older diabetic adults. A recent study by Prevent Blindness America and the National Eye Institute, demonstrated that older adult Americans are facing a bigger threat of all age-related eye diseases (diabetic retinopathy, age-related macular degeneration, cataracts and open angle glaucoma) today than at any other time.
Genetics
Our genetic make up has an important effect on our predisposition for many health issues such as diabetes. Scientists believe that many genes or combinations of genes either promote diabetes in certain individuals or protect them from developing it.
Scientists have yet to identify every gene involved in type 1 and type 2 diabetes, but they have shown that genetics are a factor. Research studies of identical twins, for instance, have demonstrated that if one twin has type 1 diabetes, the other twin has a 50 percent change of developing the disease. If one twin has type 2 diabetes, the other twin has a 75 percent chance of developing it.
Pregnancy
Gestational diabetes is a type of diabetes linked to pregnancy; however, diabetic retinopathy is usually not a complication in these women. However, if you’re already a diabetic and become pregnant, you are at an increased risk of developing diabetic retinopathy. This is a result of the hormonal and metabolic changes that occur during pregnancy, making the disease and its complications progress more rapidly. It is recommended that you see a retinal specialist for evaluation and monitoring.
In Summary
• Diabetic retinopathy is a serious complication of diabetes that results from high glucose levels damaging the retinal blood vessels. This can cause loss of vision.
• Between 40 and 45 percent of diabetic Americans have some form of diabetic retinopathy.
• The earliest form of the disease is called background diabetic retinopathy. With time it progresses to mild, moderate, or severe nonproliferative diabetic retinopathy.
• Without proper diagnosis and treatment of nonproliferative diabetic retinopathy, the condition can advance to proliferative diabetic retinopathy, which is a serious sight-threatening stage of the disease.
• Macular edema is due to build up of fluid and thickening of the macula and can occur with any type of diabetic retinopathy. It is the most common cause of vision loss in those with diabetes.
• The duration of your diabetes and how well blood glucose is controlled are major risk factors for the development and progression of diabetic retinopathy.
• Other risk factors that play a significant role in the development of retinopathy, include high blood pressure, high cholesterol, and smoking.
• As an individual with diabetes, you’re also at increased risk for other eye diseases, especially glaucoma, cataracts, retinal vein occlusion and optic nerve damage.
• Good blood sugar control, regular eye examination, and timely treatment are the key factors in reducing the damage to the eye and keeping your vision.
 Pouya N. Dayani, MD
Pouya N. Dayani, MD
Retina-Vitreous Associates Medical Group
E-Readers for Low Vision
11/18/14
While the devices mentioned in the November 13th post will help you read a hardcover or paperback book, what about an e-reader?
E-Readers for Low Vision
These lightweight portable devices come with a variety of options for people with limited vision, at a more moderate cost. The two we will look at are the Kindle and the Nook.
Kindle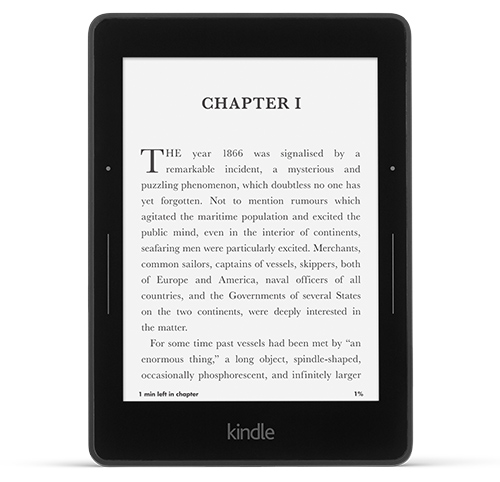
There are two options here, an e-ink reader (the Paperwhite or the new Voyage), the closest to reading a paper page, or a full-color tablet. The only accessibility options for the e-ink readers are the ability to select a font you find easy to read and the ability to increase the font size. The increase in font size is a big help, but remember, that as you increase the size you will be “turning the page” more often – the screen size is 6” diagonally. The Voyage has a whiter background than the Paperwhite allowing for more contrast. Both include a built-in screen light that can be adjusted to your needs. One thing to note is that while it does have a screen light, it is not a backlit display as you will find in the Fire HDX. This might mean less eye strain.
The Fire HDX is a full-color tablet with quite a few more accessibility options and the screen sizes range from 6” to 8.9”. Since it is a full functioning tablet you can access email, play games, watch videos and a variety of other things. It has more large-font options (that can even be used for your emails), a screen magnifier that is easily activated with a triple tap on the screen and you can pinch to adjust the zoom and the backlit display provides high contrast. There are other options for people that are blind including a screen reader to describe actions taken on your screen, five accessibility shortcut gestures to help you navigate and even Braille support with a free app from the Amazon App Store. Because it is a backlit display you may experience eye strain if you don’t occasionally take reading breaks.
Kindle also has a free accessibility plugin that is downloadable for your Windows PC. It provides the following features: text-to-speech reading, voice-guided menu navigation, large font sizes, high contrast reading mode, keyboard navigation and accessible shortcuts. It is compatible with JAWS, NVDA and Microsoft Narrator.
Nook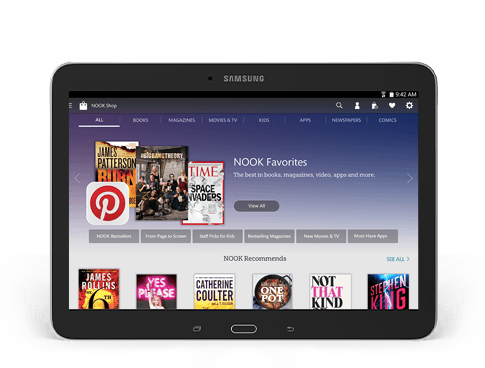
Nook, like Kindle, has two options. An e-reader called the Nook GlowLight and a full-color tablet called the Samsung Galaxy Tab 4 Nook in 7’ and 10.1” sizes. As with the Kindle e-ink reader, the only accessibility options are the font and font size. There is also a built-in light to make the page brighter.
The new full-color tablets now made by Samsung, provide you with the access of a full functioning tablet such as email, playing games, watching videos, etc. The vision accessibility options include screen magnification for the text and pictures, TalkBack which reads aloud menus and on-screen options for navigating the device, negative colors to invert the color of the screen (text that usually appears black on white will be shown white on black), color adjustment if you are color-blind, and a text-to-speech option that will allow you adjust the rate at which text is spoken and your preferred text-to-speech program. Once again, these tablets have backlit screens that may tire your eyes after an extended period of reading, so take breaks.
E-Book Formats
The Kindle and Nook each have their own proprietary book formats, meaning that you can only read a book purchased for the Kindle on a Kindle or a Nook book on a Nook, however EPUB and CBZ formats can be easily transferred to the Nook. This is more important when it comes to borrowing e-books from a library. The EPUB format is more common when e-books are offered; and while some libraries now offer Kindle books, there are more EPUB titles. If you are comfortable with technology, you can use Calibre to convert most formats into whatever format you need.
Choosing between a Kindle and a Nook is based on personal preference. You can try out both devices before you buy them at Best Buy or Staples for the Kindle and at Barnes & Noble stores for the Nook. If you already own an iPad or Android tablet, remember you can also download the free Kindle and Nook apps from the App Store or Google Play.
 Susan DeRemer, CFRE
Susan DeRemer, CFRE
Vice President of Development
Discovery Eye Foundation
For Book Lovers – Low Vision Magnifiers
11/13/14
The first of this month was Book Lover’s Day, and as an avid reader, I am willing to celebrate any day that is about reading. However, if you suffer from low vision due to age-related macular degeneration, cataracts, retinitis pigmentosa or other sight-threatening eye diseases, you may not be able enjoy reading as much as you used to.
There are several options to help you enjoy books again, including low vision magnifiers, e-books and tablets. We will provide you with a quick primer to help you select the best option for your lifestyle and budget. Today we will look at magnifiers and Tuesday we will explore e-readers and tablets.

Low Vision Magnifiers
There are several general classifications for magnifiers –
• Hand-held magnifiers – These are smaller and more portable, allowing you to read thins such as menus, price tags, prescription bottles and ingredients in addition to books. Some also come with built-in lighting that can help you see in low light situations. They can be as simple as a single glass lens to more advanced digital devices that can auto-focus, change text color and magnification or even let you snap a picture of what you are reading if steady hands are an issue. However, because of these are small enough to make them portable, the field of vision is small and reading books for any length of time might become tedious.
• Stand magnifiers – These are really better for reading books, magazines and newspapers as the field of vision is larger, your hands will not get tired holding the device and the distance between the page and the magnifier will remain more constant, making reading easier. This is especially important if you have tremors. However, these require sitting at a desk or table to be used.
• Magnifiers mounted on reading glasses – These are great for being “hands-free,” but they also limit your ability to see at varying distances, and are generally used for seeing things less than a foot from your nose.
• Video magnifiers – These devices use a video camera (similar to the portable digital device listed above) that focuses on the page and then magnifies it for viewing on a screen or monitor. Text color/background, brightness, contrast and levels of magnification can be adjusted as needed. As with the stand magnifiers, the ones able to scan an entire page of a book need to be used at a desk or table. However, now there are some machines that will even read out loud to you!
To get an idea of the range of devices available, along with the wide range of prices, here are three websites to get you started – Enhanced Vision, Optelec and Humanware.
Because each person has a different vision issue, not one magnifier works for everyone. A person with central vision loss from age-related macular degeneration will have different needs from a person with peripheral vision loss from glaucoma. That is why we suggest that you consult with a low vision specialist to help guide you in selecting the correct device for your specific needs.
Check back on Tuesday, or subscribe to the DEF blog, to learn about e-reader and tablet options for people with low vision.
Susan DeRemer, CFRE
Vice President of Development
Discovery Eye Foundation
Diabetes Awareness Month & Diabetic Eye Disease
11/11/14
Even though people with diabetes are at a greater risk of developing blinding eye diseases, a recent study of Medicare beneficiaries show that very few of the people at risk have a preventative yearly eye exam.
Facts About Diabetes
In the US there are 29.1 million that have diabetes, 21 million have been diagnosed and 8.1 million are undiagnosed. Unfortunately, if left undiagnosed or untreated, diabetes can lead to serious health problems such as high blood pressure, increased LDL cholesterol, heart disease, stroke, kidney disease and blindness.
Although African-Americans and Hispanics are more likely to have diabetes, less than a third are aware of diabetic eye disease. And for those that have been diagnosed with diabetes, where a yearly eye exam is considered essential, ¾ of them have not had an eye exam in five years.
Diabetic Eye Disease – 3 Ways Diabetes Affects Vision
Cataracts occur when there is a clouding of the eye’s lens, making your vision blurry or cloudy. While it is a normal for this to happen as a person ages, someone with diabetes is more likely to develop them at an earlier age. While beginning cataracts can be treated with glasses, when they become more advanced, cataract surgery will be needed to replace the cloudy lens with an artificial lens.
Controlling Diabetes
Diabetes can be controlled, and some cases prevented, with careful attention to diet, watching your weight and exercise. Also learn your family medical history. You are at a higher risk of diabetes if a mother, father, brother or sister has the disease. If you are diagnosed with diabetes, make sure you have a yearly comprehensive eye exam to avoid vision loss. To learn more about diabetes go to www.ndep.nih.gov.
Susan DeRemer, CFRE
Vice Pesident of Development
Discovery Eye Foundation
Living With Dry Age-Related Macular Degeneration
11/6/14
Donna Cole gives new meaning to the term lifelong learner. “I love school. I love learning,” says 79-year-old Cole, who still regularly attends classes at the Osher Lifelong Learning Institute at California State University, Long Beach. “It seems like I’ve gone to school all my life. I just love it.”
While she did not earn her college degree until she was 65, Cole excelled at jobs ranging from assistant vice president of a savings and loan association, to president of the Long Beach Committee for the 1984 Olympic Games, to assistant athletic director for Cal State Long Beach — where, incidentally, she helped raise $300,000 in a month to save the football team in the 1980s — to vice president of communications and PR for the Grand Prix Association.
It was while working as a senior systems analyst at Boeing that she earned her BA degree,  and when the company laid her off in 2003, Cole convinced them to pay for her to go back to school to earn her teaching credential. “It was the only thing I could come up with to do at my age,” she says. She earned the credential at age 70 and was a substitute teacher until her retirement in 2008.
and when the company laid her off in 2003, Cole convinced them to pay for her to go back to school to earn her teaching credential. “It was the only thing I could come up with to do at my age,” she says. She earned the credential at age 70 and was a substitute teacher until her retirement in 2008.
When her doctor diagnosed her with dry age-related macular degeneration (AMD) in 2010, she picked up a card in his office that advertised The Discovery Eye Foundation’s Vision Symposium at UC Irvine. She attended the half-day event, and she’s been “obsessed with DEF ever since. There were great speakers, and it gave me the opportunity to mingle with people at all stages of AMD,” she says, adding that she regularly attends events through DEF and the Macular Degeneration Partnership (MDP), relying on the MDP website as her primary source of AMD information.
Cole says she has yet to experience any real effects of AMD: “I’m too young for that!” she insists. “My doctor just checked me and said the same thing he says every year: ‘See you in a year’; he told me I only need to come in sooner if I notice a change in my eyesight.”
Thanks to MDP, Cole believes she is better prepared to deal with the effects of AMD when they do happen. “Knowing that support is there makes it OK,” she says. “No matter what happens, I know DEF and the Macular Degeneration Partnership are there for me.”
The California native takes an eye vitamin and mineral supplement, and she added salmon and tuna to her vegetarian diet because of their eye-healthy properties. “To me, it’s just a matter of being healthy,” Cole says. “I’m very healthy. I don’t like taking drugs — not even aspirin — but I do make sure to eat chocolate at both lunch and dinner.”
Additionally, she tries to go walking at least two or three times a week, though, recently, she laments, “I accidentally signed up for three days of classes every week this quarter, which is interfering with my walking.”
 Donna Cole
Donna Cole
Age-Related Macular Degeneration Advocate
Photophobia
11.4.14
Photophobia is a severe sensitivity to bright light which can result in discomfort and even pain. It can vary from person to person with discomfort coming from lights that don’t ordinarily affect others, including natural outdoor light, overhead lighting (such as fluorescent light), reflected light or flames of a fire.
Although in most cases photophobia is harmless, it is NOT an eye disease, but may be a symptom of an underlying problem. These could include an infection or abrasion that irritates the eye, a viral illness, medications, severe headache or migraine. 
It could also be the result of your unique physical makeup. A person’s eye color can also affect ones sensitivity to light. People with lighter colored eyes can be more sensitive to light as opposed to people with darker eyes. An examination by an eye doctor can help determine the cause of your sensitivity.
The best treatment option for relieving the discomfort of photophobia is to address the underlying cause. The answer may be as simple as changing a medication or treating a corneal abrasion. Or your photophobia could be the clue that alerts doctors to another treatable condition. If you are naturally sensitive to light, wearing sunglasses with UV protection, brimmed hats or avoiding bright light situations are the only alternatives. In most cases, if you treat the underlying cause, the sensitivity will decrease or disappear.
Susan DeRemer, CFRE
Vice President of Development