
Many children who are 6 – 18 years old are now back in school or will be shortly. But have you given them everything they need to succeed in the school year ahead?
? New binders
? Notebook paper and dividers
? Pencil box filled with pens and pencils
? Calculators, protractors and rulers
? Backpack to carry it all
These are the tools that children and their parents focus on every year, thinking these will help their child have a fun and productive year. But the list is incomplete. For school-aged children, the AOA recommends eye exams for children every two years if no vision correction is required. Children who need eyeglasses or contact lenses should be examined annually or according to their eye doctor’s recommendations.
“But my child gets and eye screening at school every year…” While this may be true it is important to understand the difference between a screening and an eye exam.
Vision screenings are a short examination that can indicate a vision problem or a potential vision problem; however it cannot diagnose exactly what is wrong with your eyes. It can also easily miss vision issues, giving parents a false sense of security.
With an eye exam, the tests are performed by a trained professional, using specialized equipment looking for specific indicators that could affect your child’s vision. They test much more than how well your child can read letters or symbols at a distance.
Good vision is necessary for a child to succeed at school and not become frustrated or depressed. It has been estimated that as much as 80% of the learning a child does occurs through his or her eyes. Children need to read a book and see a whiteboard, write and use computers every day in the classroom and at home. When a child cannot see clearly, it becomes more difficult to learn.
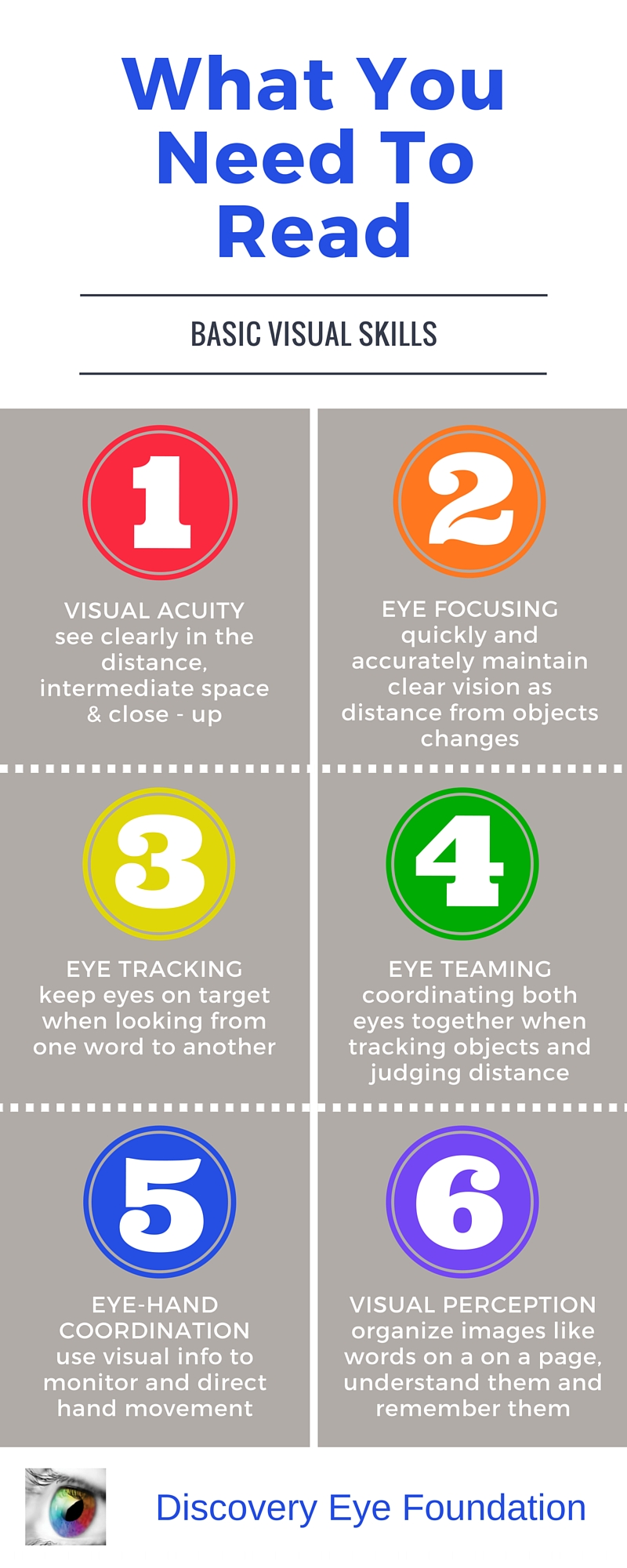
It also goes beyond just seeing clearly. Your child needs their eyesight to understand and respond to what they see. This includes the ability to focus their eyes, use both eyes together, and move them effectively.
Children may not always know they have a vision problem because they think that everyone is seeing the way they do. There are some signs that may indicate a vision issue:
- Repeated eye rubbing
- Excessive blinking
- Short attention span
- Tilting the head to one side or covering one eye
- Holding reading materials too close to the face
- Losing their place when reading
- Difficulty remembering what they just read
- Trying to avoid reading or other close activities
- Numerous headaches
So as you prepare your child to go back to school, give them the best advantage they can have – good vision. Make an appointment with your eye doctor today.
8/27/15
 Susan DeRemer, CFRE
Susan DeRemer, CFRE
Vice President of Development
Discovery Eye Foundation















