A healthy diet not only helps your heart, but also your eyes. Your diet should include lots of fruits and vegetables to provide you with a natural source of nutrients to help protect your sight. As wonderful as supplements are, eating the actual foods is always better. Some of the best vegetables for you are the dark, leafy greens that are rich in valuable vitamins and nutrients. These are the super greens for better sight.
With the US experiencing bitter, freezing temperatures on the East Coast, while the West Coast is having summer in February, with record-breaking hot temperatures, I thought it would be interesting to see how you could enjoy those super greens, no matter what the temperature is outside. Below is a quick look at four dark leafy greens that are a great addition to a healthy diet, watercress, arugula, spinach and kale. For each vegetable I have included a recipe that is served hot, along with one that is served cold.
Here is what you need to know about super greens for better sight.

WATERCRESS
Watercress is a cruciferous plant and part of the brassica family, like arugula and kale. It contains vitamins A, B6, B12, C, K, iron, magnesium, calcium, phosphorus, lutein and zeaxanthin. In fact, weight for weight, watercress contains more vitamin C than an orange, more calcium than milk, more iron than spinach and more folate than bananas. Watercress has the highest amount of nutrients for the smallest amount of calories.
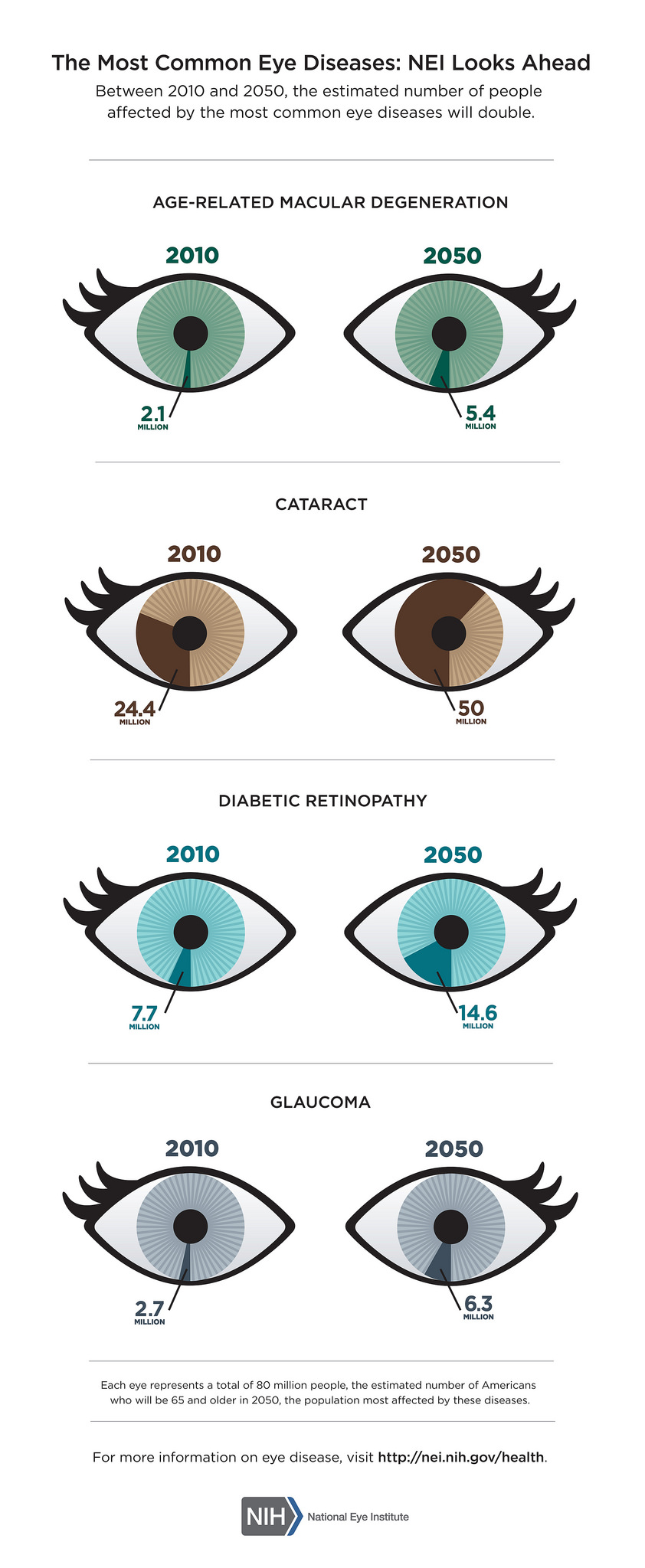
The health benefits of watercress include boosting immunity, cancer & diabetes prevention, reducing cognitive decline, thyroid support, better cardiovascular health and stronger bones. As for your eyesight, it can help prevent or slow the onset of age-related macular degeneration and possibly cataracts.
Watercress is most commonly enjoyed fresh in salads, but can also be use in pastas, casseroles, soups and sauces. Choose watercress with deep green, crisp leaves, with no signs of wilting. Trim the stems, rinse the greens in cold water and dry. It is best if used immediately, but can be store for up to four days in the refrigerator.
Watercress Soup by William Anatooskin
Watercress and Grapefruit Salad by Martha Stewart

ARUGULA
Arugula is also known as a salad or garden rocket. It is a small low growing herb that is packed with vitamins, minerals and antioxidants. It is rich in folates, vitamin A, B-complex, C and K and has copper, iron, calcium, potassium, manganese and phosphorus.
The health benefits of arugula include a lowered risk of cancer, healthy bones, strengthened brain function, improved mineral absorption and it boosts the immune system. Because of being a source of carotenoids, it also helps to slow the progression of age-related macular degeneration.
Arugula is popular in salads, used with milder greens to add a peppery flavor. But it can also be used in pastas, casseroles, pizzas, soups and sauces. Choose arugula that is crisp with green young leaves. Avoid the flowered harvest as those leaves are tough and have a bitter taste. Wash leaves in a bowl of water, swishing thoroughly to get rid of all sand and soil. Drain and pat dry before storing in the vegetable bin of your refrigerator for no more than a few days.
Grilled Stuffed Swordfish by Stormy Scarlett
Pasta Salad with Goat Cheese and Arugula by Martha Stewart

SPINACH
Spinach is a very popular leafy green vegetable, with two common varieties cultivated for food; the savory-type with dark green crinkled leaves and the flat-leaf type with smooth surfaced leaves. Spinach contains vitamin A, B-complex, C and K, along with lutein, zeaxanthin beta-carotene, potassium manganese, magnesium, copper and zinc.
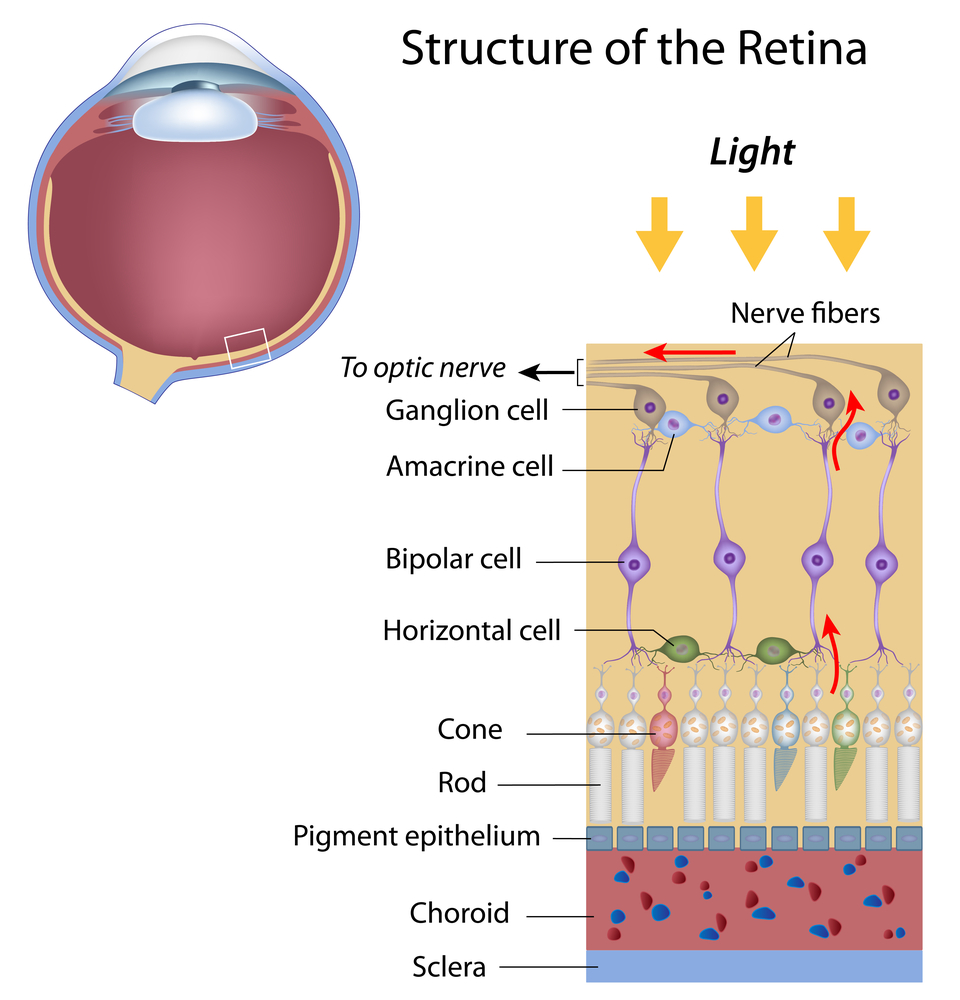
The nutrients in spinach help improve blood glucose control in diabetes, lower the risk of certain cancers, reduce blood pressure, increase bone health and help iron deficiency. The lutein, zeaxanthin and beta-carotene help to potentially prevent and slow the progression of age-related macular degeneration. Lutein also works to protect the eye from free radical damage by helping filter out damaging blue and ultraviolet light.
Spinach is a universally popular vegetable, used around the world in a variety of ways, including salads, soups, noodles, pies, casseroles, dips, sauces, etc. Look for leaves that are dark green in color, crisp and not dull or yellow and spotted. Wash thoroughly to remove sand and soil, dry, trim away tough stems and store in the refrigerator for up to a week.
Turkey-Spinach Meatballs from Bon Appètit
Spinach Salad with Dates from Bon Appètit

KALE
Kale is a member of the mustard and cabbage families and has more nutrients than spinach. Less than ½ cup has 333% of the recommended daily allowance (RDA) of vitamin A, 587% RDA of vitamin K and 200% RDA of vitamin C. This frilly-leafed vegetable also has vitamin B-complex, lutein, zeaxanthin, beta-carotene, copper, calcium, sodium, potassium, iron, manganese, and phosphorus.
The health benefits of kale include healthy muscles and skin, improved blood glucose control, lower colon and prostate cancer risk, better cardiovascular health, stronger bone health, reduced neuronal brain damage and support for red blood cell formation. The advantage for your eyes comes from the lutein, zeaxanthin, beta-carotene and vitamin A, all which work to support a healthy retina. They help protect against blue and ultraviolet light as well as the early onset and progression of age-related macular degeneration. Because of the positive impact on diabetes it also reduces the onset and progression of diabetic retinopathy.
Kale is very versatile and can be served in a variety of ways including salads, soups and casseroles. It can also be braised, broiled, sautéed and even made into kale chips by tossing them in extra-virgin olive oil and sprinkled with your choice of cumin, curry powder, chili powder, red pepper flakes or garlic powder and baking at 275 degrees for 15-30 minutes depending on how crisp you want them to be. When shopping for kale look for leaves that are crispy and crunchy with a brilliant dark blue-green color. Wash thoroughly to remove soil and sand, dry well, and remove all tough stems. It is extremely perishable, so use it as quickly as possible.
Kale and Chicken Casserole by Martha Stewart
Kale with Pomegranate Dressing and Ricotta Salata from Bon Appètit
All of these dark green leafy vegetables are not only healthy for you, but can be used in many ways to make it easy to incorporate them into your diet. Here are a few ideas:
- Throw a small handful into your blender when making your favorite smoothie
- Add them to your next omelet or egg scramble
- Use them for making pesto or adding to pasta sauce
- Sauté with a small amount of extra-virgin olive and season with freshly ground black pepper and freshly grated Parmesan cheese to serve at a topping for your baked potato
- Add it to your wrap, sandwich or flatbread
2/17/16
 Susan DeRemer, CFRE
Susan DeRemer, CFRE
Vice President of Development
Discovery Eye Foundation