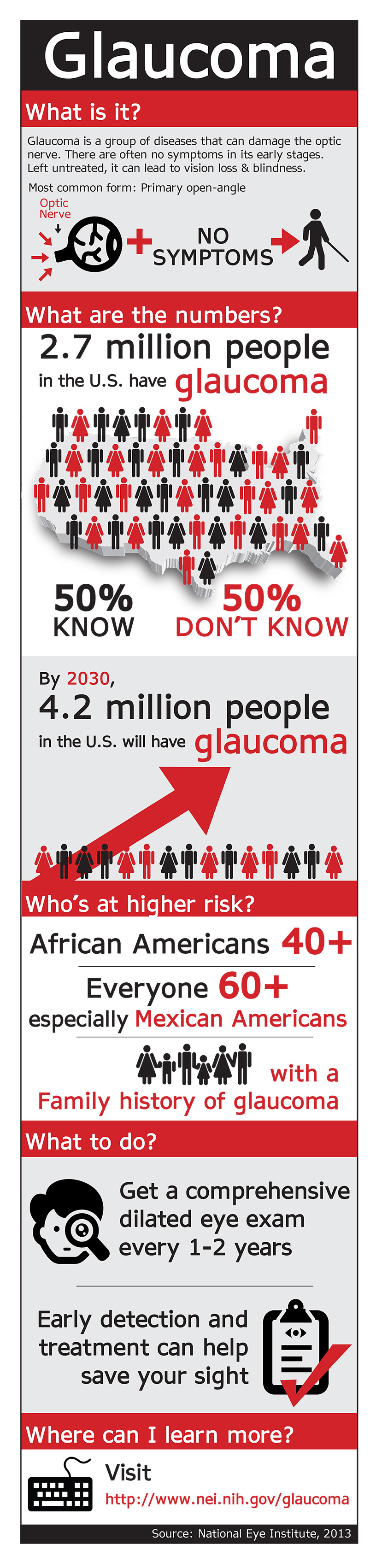
Did you know January is Glaucoma Awareness Month? Although no cure exists, the eye disease may be treated with medication and surgery. If left undiagnosed and untreated, however, glaucoma can cause permanent damage to vision. According to the National Eye Institute, glaucoma affects more than three million people in the United States. The population that is at highest risk is adults over the age of 60. Glaucoma affects vision by damaging the optic nerve and typical vision loss occurs in the peripheral visual field. This type of loss can create difficulty performing everyday tasks. To mark the importance of Glaucoma Awareness Month, Low Vision Focus @ Hadley offers these tips to improve independence and safety for people with glaucoma-related vision impairments.
Tips for Living With Glaucoma
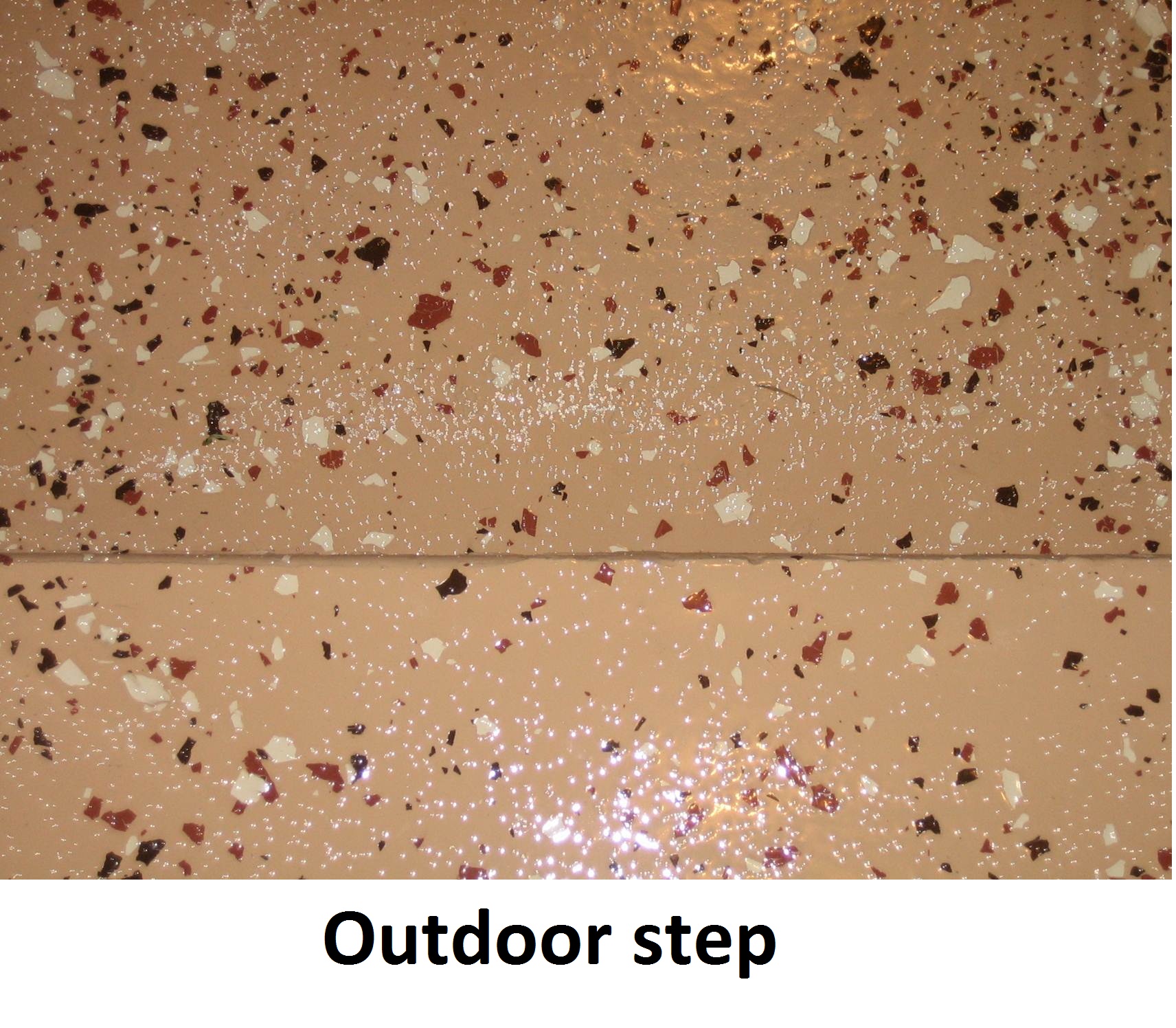
- Loss of peripheral vision makes it difficult to see steps and stairways. Marking treads and handrails with contrasting colored paint or tape can improve navigation and reduce the risk of falling.
- Persons with glaucoma often experience difficulty adjusting to darkness or darkened rooms. Increase illumination in dark closets or hallways by installing additional lighting fixtures. When outdoors at night, carry a strong flashlight.
- Area rugs can pose a hazard for persons with visual field loss. It’s best to keep home pathways and work areas free of extra floor coverings.
- In all locations where you might be a frequent visitor, ask someone to give you a tour. It goes without saying you need to know where the bathroom is located, as well as how to exit the building from a variety of locations.
- Some persons with glaucoma prefer to use a human guide when traveling in unfamiliar places. To use a human guide effectively, grasp the guide’s arm firmly just above the elbow and walk a half a step behind. This positioning gives the most protection from potential obstacles and allows both people to function as a team.
- Get in the habit of consistently closing kitchen and bathroom cabinets, especially those above countertops. Make sure doors are either all the way open or shut. Practicing both of these safety techniques can greatly reduce the risk of head injury.
- Before reaching down to pick up dropped objects, place your hand, palm out, about 12 inches in front your face. This way, you’ll make sure you don’t hit the edges of tables or countertops with your forehead.
Remember, although glaucoma cannot be cured, it can be treated. Regular eye exams, especially for adults over 60, are critical to control the spread of the disease. For those who are affected by vision loss, it’s important to remember that the acquisition of some simple adaptive skills and techniques can help maintain safety and independence. Low Vision Focus@Hadley is dedicated to assisting persons with low vision to live life to the fullest all year long. For more information on how Low Vision Focus@Hadley can help you or someone you know, please visit our website www.lowvisionfocus.org, or call (855) 830-5355 to find out about our free programs and materials.
1/12/16
 Ed Haines
Ed Haines
The Hadley School for the Blind
Low Vision Focus @ Hadley