Harsh weather conditions can reduce the natural moisture in your eyes and the irritation usually results in a burning or itching sensation that often leads to rubbing or scratching your eyes which can worsen the symptoms. Sometimes it feels like there is a foreign object in your eye and for some, dry eyes can even cause excessive tearing, as your eyes try to overcompensate for their lack of protective tears. Prolonged, untreated dry eyes can lead to blurred vision as well. Between the harsh winter winds outside and the dry heat radiating inside, our eyes are very quickly irritated and dried in the winter months. The result is itchy, dry eyes that may cause pain, blurred vision, a burning sensation, or even watery vision as our eyes try to compensate for the dryness.
Harsh weather conditions can reduce the natural moisture in your eyes and the irritation usually results in a burning or itching sensation that often leads to rubbing or scratching your eyes which can worsen the symptoms. Sometimes it feels like there is a foreign object in your eye and for some, dry eyes can even cause excessive tearing, as your eyes try to overcompensate for their lack of protective tears. Prolonged, untreated dry eyes can lead to blurred vision as well. Between the harsh winter winds outside and the dry heat radiating inside, our eyes are very quickly irritated and dried in the winter months. The result is itchy, dry eyes that may cause pain, blurred vision, a burning sensation, or even watery vision as our eyes try to compensate for the dryness.
What Are The Symptoms?
- Uncomfortable, stingy, burning or scratchy feeling.
- Stringy mucus in or around your eyes
- Increased eye irritation from smoke or wind
- Eye fatigue
- Sensitivity to light
- Eye redness
- A sensation of having something in your eyes
- Difficulty wearing contact lenses
- Periods of excessive tearing
- Blurred vision, often worsening at the end of the day or after focusing for a prolonged period
10 TIPS TO KEEP YOUR EYES COMFORTABLE DURING THE WINTER MONTHS
Whatever the symptoms, dry eyes can cause significant discomfort during the long winters and relief can seriously improve your quality of life.
- To keep eyes moist, apply artificial tears/eye drops a few times a day. If you have chronic dry eyes, speak to your eye doctor about the best product for your condition.
- Drink a lot of fluids – keeping your body hydrated will also help maintain the moisture in your eyes.
- If you spend a lot of time indoors in heated environments, use a humidifier to add some moisture back into the air.
- Try to situate yourself away from sources of heat, especially if they are blowing. While a nice cozy fire can add to the perfect winter evening, make sure to keep your distance so dry eyes don’t ruin it.
- Staring at a computer or digital device for extended amounts of time can further dry out your eyes. If you spend a lot of time staring at the screen, make sure you blink often and practice the 20/20/20 rule – every 20 minutes, look 20 feet away for 20 seconds. Use artificial tears often to lubricate eyes during long periods of using your eyes.
- Avoid air blowing in your eyes. Don’t direct hair dryers, car heaters, air conditioners or fans toward your eyes. In your car, direct heat to floor vents and away from your eyes once your windshield is defrosted.
- Stop smoking and avoid smoky environments.
- Don’t rub your eyes! This will only increase irritation and can also lead to infections if your hands are not clean.
- Give your eyes a break and break out your glasses. If your contact lenses are causing further irritation, take a break and wear your glasses for a few hours or days. Also talk to your optometrist about switching to contacts that are better for dry eyes.
- Protect your eyes. If you know you are going to be venturing into harsh weather conditions, such as extreme cold or wind, make sure you wear protection. Try large, 100% UV protective eyeglasses and a hat with a visor to keep the wind and particles from getting near your eyes. If you are a winter sports enthusiast, make sure you wear well-fitted ski goggles.
If you find that after following these tips you continue to suffer, contact your eye doctor.
 Most people have eye problems at one time or another. Some are minor and will go away on their own, or are easy to treat at home. Others need a specialist’s care. Some eye issues come with age while others may be a serious condition.
Most people have eye problems at one time or another. Some are minor and will go away on their own, or are easy to treat at home. Others need a specialist’s care. Some eye issues come with age while others may be a serious condition.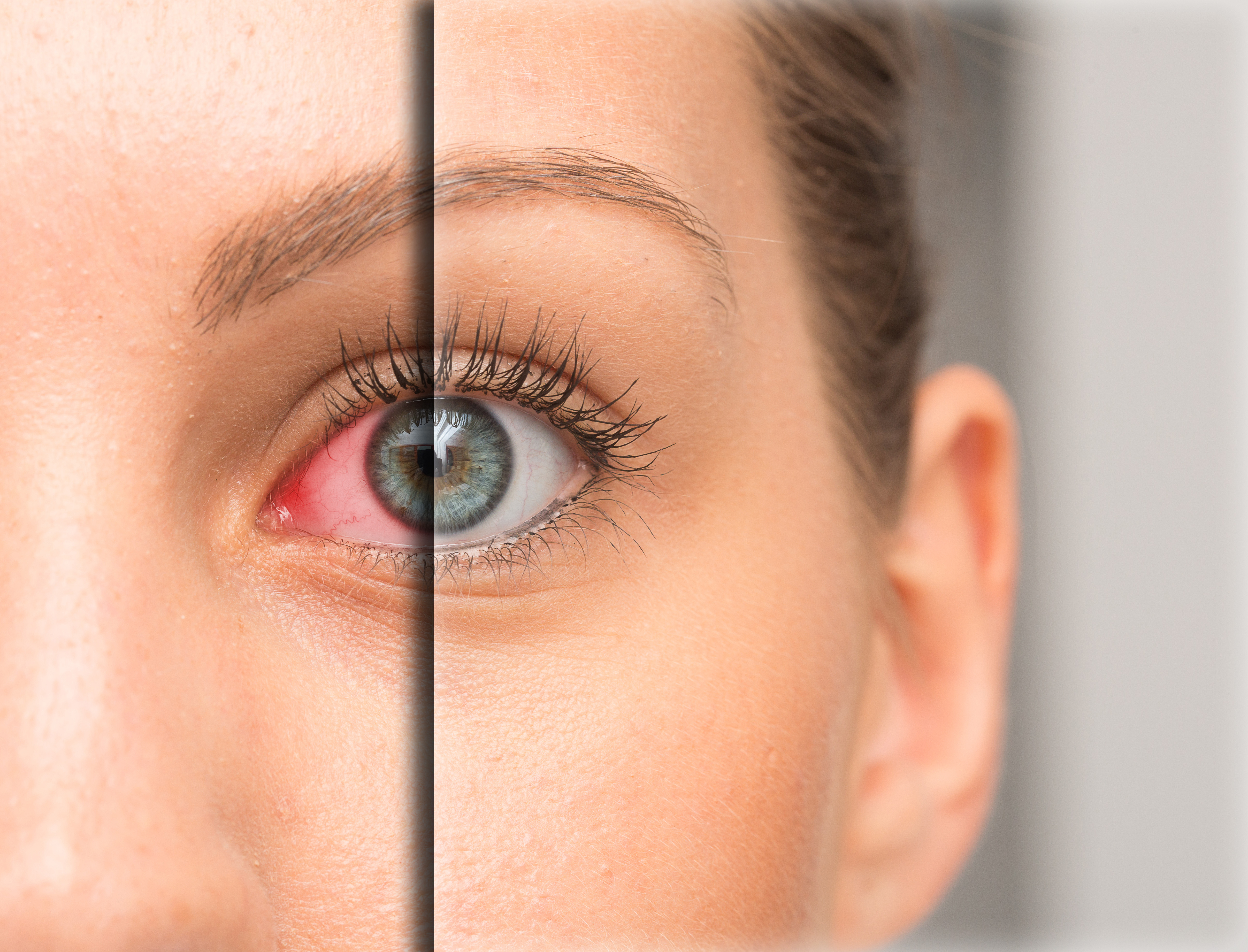 Dry eye is a common condition that occurs when your tears aren’t able to provide adequate lubrication for your eyes. Tears can be inadequate for many reasons. For example, dry eyes may occur if you don’t produce enough tears or if you produce poor-quality tears. Dry eyes can also feel very uncomfortable.
Dry eye is a common condition that occurs when your tears aren’t able to provide adequate lubrication for your eyes. Tears can be inadequate for many reasons. For example, dry eyes may occur if you don’t produce enough tears or if you produce poor-quality tears. Dry eyes can also feel very uncomfortable.

 UV Protection – Sunglasses for children should block 100% of UV radiation as well as between 75 – 90% of visible light. Any sunglasses you buy should have this information provided in the packaging
UV Protection – Sunglasses for children should block 100% of UV radiation as well as between 75 – 90% of visible light. Any sunglasses you buy should have this information provided in the packaging