If you need eyeglasses it is because you were diagnosed with a refractive error during your eye exam. This means your eyes have trouble focusing and images can appear blurry. Types of refractive errors include being near-sighted (myopia), far-sighted (presbyopia) or having an astigmatism (your cornea is an irregular shape).
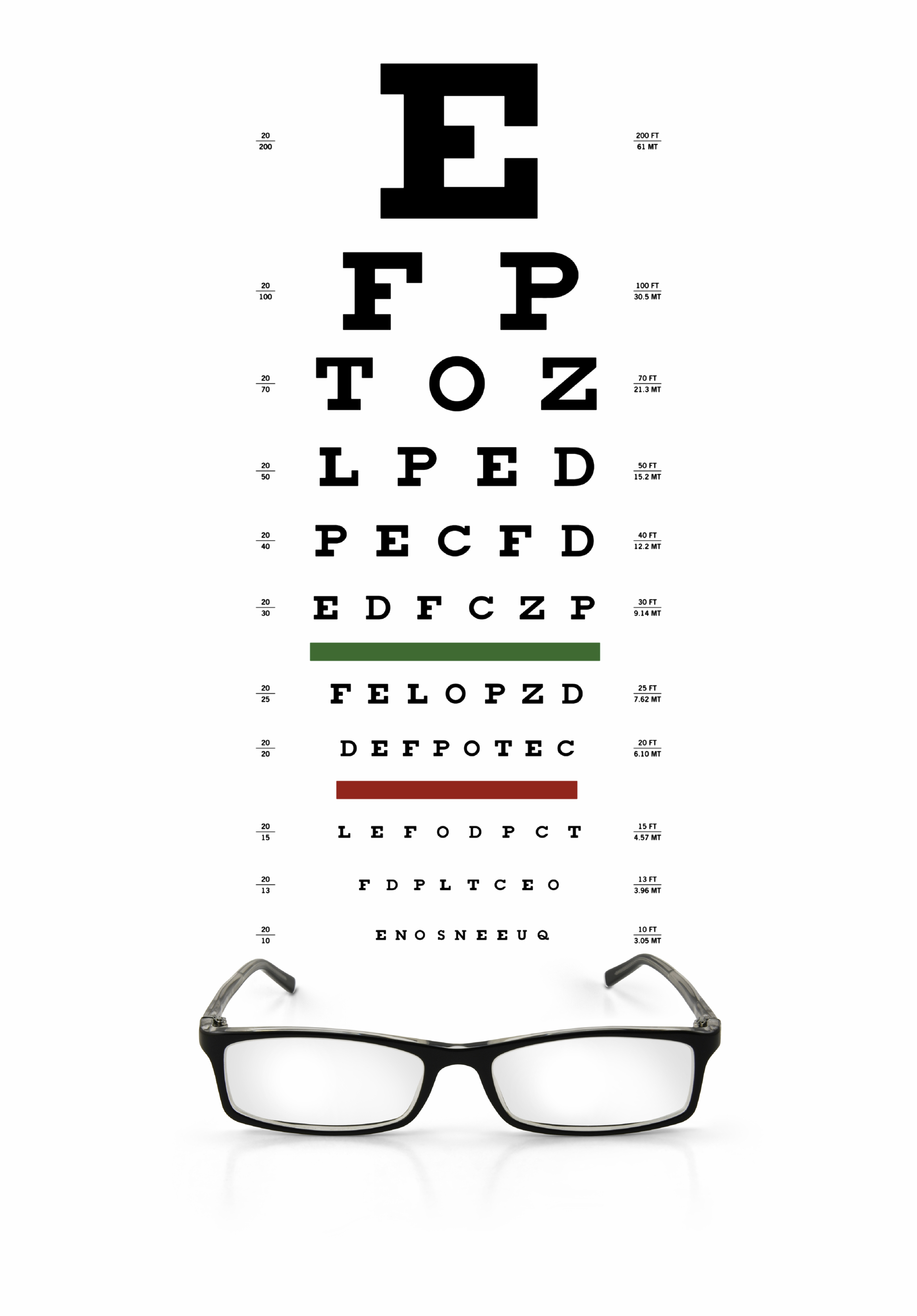
Understanding What 20/20 Vision Means
The number is based on you standing a distance of 20 feet (considered to be the norm) in front of a Snellen or Tumbling E eye chart to test your visual acuity. If during an eye test you can read the big E at the top of the eye chart, but none of the letters below that, your vision is considered 20/200. That means you can read a letter at 20 feet that people with “normal” vision can read at 200 feet, meaning you have very poor visual acuity. If you can read the fourth line from the bottom of most charts, you vision is 20/20. Any line below that would be 20/15 or below and indicates that you have exceptional visual acuity. Each eye is tested separately as your eyes are designed to compensate for each other and would not give an accurate reading.
Understanding Your Eyeglass Prescription
The prescription you receive may be a chart with headings that are filled in, or it may just be written out. In any case, it is written in a specific order, with the results for each eye listed first.
- OD is an abbreviation for oculus dexter, meaning right eye, while OS is oculus sinister, meaning left eye. If both eyes are being referred to the abbreviation you will see is OU (oculus uterque) meaning both eyes.
- The next term on your prescription is Sphere (SPH) and is are measured in diopters (D). This number tells you how strong your lenses need to be to correct your vision. If this number has a minus sign (–), you are nearsighted; if the number has a plus sign (+) or is not preceded by any sign, you are farsighted.
- Next may be cylinder (CYL), an indicator of the lens power if you have an astigmatism. The number for the CYL has the same format as the SPH, a minus sign (for the correction of nearsighted astigmatism) or a plus sign (for the correction of farsighted astigmatism). If there is no number given you either have no astigmatism, or your astigmatism is so slight that it is not really necessary to correct it.
- If you do have a CYL number you will also have an axis number, based on a protractor scale that tells you where on the eye the astigmatism is found. For example, SPH –2.50 D CYL +5.00 Axis 40 means you have a nearsightedness of -2.50 dioptics with an astigmatism of +5.00 along the 40 degree axis.
- If you are getting bifocals or progressive lenses, there is another number called an “Add.” This number is the amount of additional correction your eyes need to focus at close distance and will always be a positive number, whether or not the + sign is there.
Needless to say, eyeglasses are expensive, but understanding a prescription should help you understand why. The stronger the lens the more expensive it is and then with each adjustment, the cost also increases. Also don’t forget that anti-glare or UV protective coatings add to the costs, but may be well worth it. Eye glasses are an investment in your safety, job, independence and letting you enjoy any leisure-time activities you enjoy.
2/9/16
 Susan DeRemer, CFRE
Susan DeRemer, CFRE
Discovery Eye Foundation