All of us are players in the human drama, and there are moments when we get to observe it up close and very personal. I was in Chicago, preparing to speak in an ophthalmology practice. As I often do, I arrived early to sit in the waiting area and work to get a feel for the energy and style of the practice. I didn’t mean to overhear their conversation, but as I listened, I was deeply touched by their love and in that moment, their fear.
I learned that Charlie was 88 and Rose was 86. I am sure they were holding hands as Rose was saying “Oh, Charlie, I am so sorry about the falls I have had. I just can’t see the step from the kitchen into the family room.”
Charlie tried to comfort her. “It’s alright Dear, the Doctor will give us the answers, and I am sure you’ll be better.”
I didn’t speak to Charlie over the next 40 minutes believing that I would be intruding but sure that he was living every second of the exam going on just a few steps away.
When Rose exited the Doctor’s office, she was supported by the Doctor and a Tech who must have been holding her up because she collapsed into her husband’s arms.
“I’m sorry,” she kept saying. “I am sorry Charlie. It’s Macular Degeneration. And, the Doctor says there’s very little he can do for me.”
 I could hear Charlie rubbing his wife’s shoulders and telling her that everything would be alright. But, Rose kept saying “I know we’ll have to sell the house and move into something smaller, and I am going to be blind Charlie. Blind.”
I could hear Charlie rubbing his wife’s shoulders and telling her that everything would be alright. But, Rose kept saying “I know we’ll have to sell the house and move into something smaller, and I am going to be blind Charlie. Blind.”
Moments like this are happening across the country in ophthalmology and optometry practices every day. 30% of adults, age 60 and older, suffer from this horrible disease, and only through research will answers be found.
The Discovery Eye Foundation is committed to finding those difficult answers and making it possible for people like Rose to see the faces of loved ones for many years to come.
 Tom Sullivan
Tom Sullivan
DEF’s Ambassador of Vision
sullivanvision.com
 Today, people are living longer than ever before so it’s important to be proactive and take responsibility for your health as you age.
Today, people are living longer than ever before so it’s important to be proactive and take responsibility for your health as you age. 
 Maintain a healthy weight. Being overweight increases your risk for diabetes. By exercising regularly, you can help keep your body healthy and prevent vision loss.
Maintain a healthy weight. Being overweight increases your risk for diabetes. By exercising regularly, you can help keep your body healthy and prevent vision loss.  Don’t smoke. Smoking increases your risk for age-related macular degeneration, cataract, and other eye diseases and conditions that can damage the optic nerve.
Don’t smoke. Smoking increases your risk for age-related macular degeneration, cataract, and other eye diseases and conditions that can damage the optic nerve. Wear protective eyewear when outdoors. Protecting your eyes from the sun’s ultraviolet rays when you are outdoors is vital for your eye health. Wearing sunglasses that block 99 to 100 percent of both UV-A and UV-B radiation.
Wear protective eyewear when outdoors. Protecting your eyes from the sun’s ultraviolet rays when you are outdoors is vital for your eye health. Wearing sunglasses that block 99 to 100 percent of both UV-A and UV-B radiation. Know your family history. Talk to your family members about their eye health history. It’s important to know if anyone has been diagnosed with a disease or condition since many are hereditary, such as glaucoma, macular degeneration, and diabetes . This will help determine if you are at higher risk for developing an eye disease or condition.
Know your family history. Talk to your family members about their eye health history. It’s important to know if anyone has been diagnosed with a disease or condition since many are hereditary, such as glaucoma, macular degeneration, and diabetes . This will help determine if you are at higher risk for developing an eye disease or condition. Consider a multivitamin. Vitamins C, E and the mineral zinc have been shown to promote eye health. Vitamins with Lutein and Zeaxanthin have been known to help patients with moderate to severe age-related macular degeneration.
Consider a multivitamin. Vitamins C, E and the mineral zinc have been shown to promote eye health. Vitamins with Lutein and Zeaxanthin have been known to help patients with moderate to severe age-related macular degeneration. Give your eyes a rest. If you spend a lot of time at the computer or focusing at any one distance, you sometimes forget to blink, resulting in dryness and eye fatigue. Every 20 minutes, look away about 20 feet in front of you for 20 seconds. This can help reduce eyestrain. Consider using a lubricant eye drop during long periods of intense eye use and rest your eyes for 5 minutes.
Give your eyes a rest. If you spend a lot of time at the computer or focusing at any one distance, you sometimes forget to blink, resulting in dryness and eye fatigue. Every 20 minutes, look away about 20 feet in front of you for 20 seconds. This can help reduce eyestrain. Consider using a lubricant eye drop during long periods of intense eye use and rest your eyes for 5 minutes.
 Tom Sullivan
Tom Sullivan





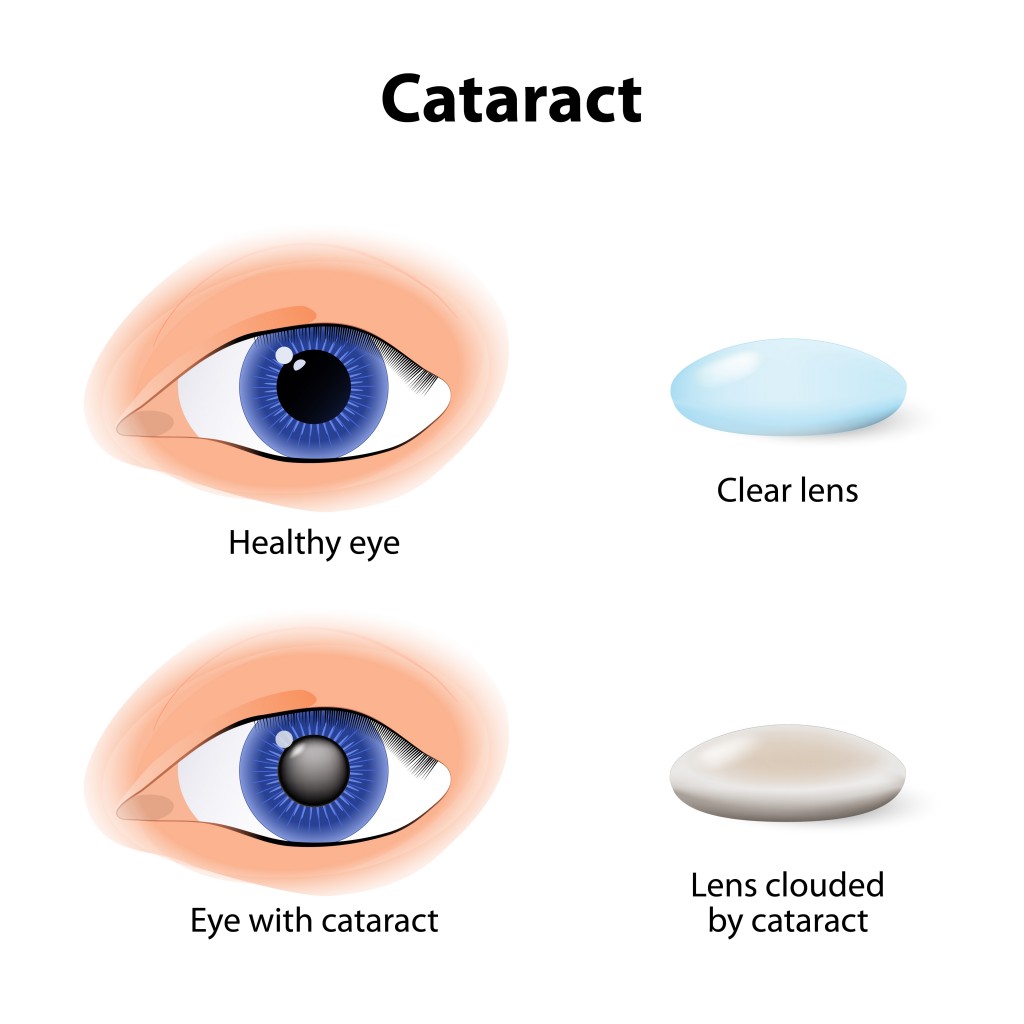
 The Difference Between an
The Difference Between an 
 Be sure to start your holiday meal with a salad, it’s an excellent way to ensure that you and your guests get plenty of zeaxanthin and lutein, two nutrients that help protect your central vision. Adding kale, spinach, or romaine lettuce to salads helps your eyes absorb damaging blue light, combats the effects of cigarette smoke and pollution, and also decreases your risk of developing
Be sure to start your holiday meal with a salad, it’s an excellent way to ensure that you and your guests get plenty of zeaxanthin and lutein, two nutrients that help protect your central vision. Adding kale, spinach, or romaine lettuce to salads helps your eyes absorb damaging blue light, combats the effects of cigarette smoke and pollution, and also decreases your risk of developing  Turkey and lean beef, two of the main ingredients in many holiday meals, keep your eyes strong and healthy. Both foods are high in zinc, a nutrient important to the retina and the choroid layer under the retina.
Turkey and lean beef, two of the main ingredients in many holiday meals, keep your eyes strong and healthy. Both foods are high in zinc, a nutrient important to the retina and the choroid layer under the retina.  Zinc is essential for good night vision. Eating foods that are high in the nutrient can also reduce your risk of cataracts and AMD. Other foods that contain zinc include pork, dairy products, chick peas, black-eyed peas, crab, oysters, beans, spinach, mushrooms, cashews, and almonds.
Zinc is essential for good night vision. Eating foods that are high in the nutrient can also reduce your risk of cataracts and AMD. Other foods that contain zinc include pork, dairy products, chick peas, black-eyed peas, crab, oysters, beans, spinach, mushrooms, cashews, and almonds.  It wasn’t an old wives tale, it is true Carrots are good for your eyes! They contain beta carotene, a substance that turns into vitamin A when eaten. Eating carrots can benefit your night vision and could possibly reduce your risk of cataracts, AMD, and dry eyes. Other foods that contain beta carotene include pumpkin, sweet potatoes, and butternut squash. All great ingredients to include into your holiday feast.
It wasn’t an old wives tale, it is true Carrots are good for your eyes! They contain beta carotene, a substance that turns into vitamin A when eaten. Eating carrots can benefit your night vision and could possibly reduce your risk of cataracts, AMD, and dry eyes. Other foods that contain beta carotene include pumpkin, sweet potatoes, and butternut squash. All great ingredients to include into your holiday feast.  Fish contain omega-3 fatty acids, which can reduce your risk of developing AMD, dry eye, and glaucoma. Salmon, mackerel, flounder, tuna, halibut, herring, and sardines would be a great addition to your holiday meals.
Fish contain omega-3 fatty acids, which can reduce your risk of developing AMD, dry eye, and glaucoma. Salmon, mackerel, flounder, tuna, halibut, herring, and sardines would be a great addition to your holiday meals. Whole grains reduce your risk of heart disease, obesity, and type 2 diabetes and can also decrease your risk of AMD. Substituting whole grain flour for white flour in holiday breads and muffins is a simple way to boost your whole grain intake. Other good whole grain sources include wild rice, brown rice, popcorn, oatmeal, bulgur, barley, buckwheat, and couscous.
Whole grains reduce your risk of heart disease, obesity, and type 2 diabetes and can also decrease your risk of AMD. Substituting whole grain flour for white flour in holiday breads and muffins is a simple way to boost your whole grain intake. Other good whole grain sources include wild rice, brown rice, popcorn, oatmeal, bulgur, barley, buckwheat, and couscous.  Fruits high in vitamin C, such as strawberries and oranges, also offer important vision benefits. Vitamin C is an antioxidant, a substance that can prevent cell damage caused by free radicals. Vitamin C-rich foods help keep the collagen in your cornea healthy and reduce the risk of cataracts and AMD. You can also find vitamin C in grapefruit, kiwi, blueberries, peas, broccoli, and tomatoes.
Fruits high in vitamin C, such as strawberries and oranges, also offer important vision benefits. Vitamin C is an antioxidant, a substance that can prevent cell damage caused by free radicals. Vitamin C-rich foods help keep the collagen in your cornea healthy and reduce the risk of cataracts and AMD. You can also find vitamin C in grapefruit, kiwi, blueberries, peas, broccoli, and tomatoes.