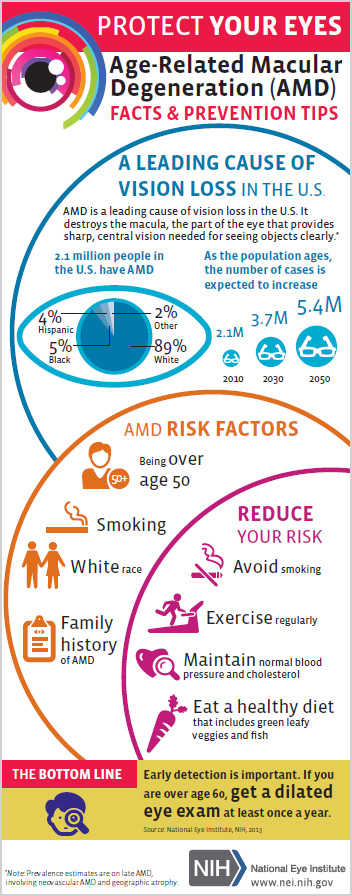
Lately we have heard quite a bit about carrots and the positive effects they can have on your vision, such as slowing the progression of age-related macular degeneration (AMD). This is because carrots contain pigments called carotenoids. These pigments also give vegetables their colors, in this case orange. But carrots weren’t always orange.
The beginnings of carrots can be tracked back to the dry, hot lands of Iran and Afghanistan in 3000 BC, when the root vegetables were black, white, red and purple. They were bitter and used as a healing remedy for many illnesses, as well as an aphrodisiac.

The vegetable grew in popularity because it was still edible even after months of being stored in a variety of conditions. Carrot seeds were soon picked and sold to neighboring Middle Eastern, African and Asian populations. This is when the crossbreeding started and new types of carrots were created.
Across centuries and continents, the carrot evolved, improving the composition, look, flavor and size. After years of selective breeding, in the 17th century a Dutch yellow carrot was engineered to get rid of the bitterness, increase sweetness and minimalize the wooden core. This appears to be the origin of the orange carrot we enjoy today.
Americans didn’t fully use carrots until after World War I when soldiers returning home told about French and other European cuisine which included the carrot. However, it didn’t really become popular until World War II, when England actively encouraged home growing of carrots while the US was engaged in cultivating “Victory Gardens.”
Today the carrot is found around the world in temperate regions. They have a high nutrition value, presence of ?-carotene, dietary fiber, antioxidants, minerals and ability to be prepared in a wide variety of recipes. They have become a staple in many countries.
Currently, the largest producer and exporter of carrots in the world is China. In 2010, 33.5 million tons of carrots and turnips were produced worldwide, with 15.8 million tons from China, 1.3 million tons each from the US and Russia, 1 million tons from Uzbekistan and less than a million from Poland, the United Kingdom and Ukraine.
Because of the popularity and health benefits of carrots, they are now enjoyed in a variety of ways – beyond the simple salad. Here are some recipes you might find interesting to try:
 Crab Toast with Carrot and Scallion – Forget your traditional bruschetta, wow your guests with the appetizer.
Crab Toast with Carrot and Scallion – Forget your traditional bruschetta, wow your guests with the appetizer.
 Potato-Carrot Latkes with Lemon-Raisin Topping – Seems perfect with Hanukkah just around the corner.
Potato-Carrot Latkes with Lemon-Raisin Topping – Seems perfect with Hanukkah just around the corner.
 Roasted Carrot, Squash and Sweet Potato Soup – This is a more traditional carrot recipe, it is not that hard to find a carrot soup, but this one also has squash and sweet potatoes which are also eye healthy!
Roasted Carrot, Squash and Sweet Potato Soup – This is a more traditional carrot recipe, it is not that hard to find a carrot soup, but this one also has squash and sweet potatoes which are also eye healthy!
 Carrot Farfalle Pasta with Lemon and Herbs – Not only are carrots good for flavor, but they add a nice color to this pasta that could be the base for any number of pasta dishes.
Carrot Farfalle Pasta with Lemon and Herbs – Not only are carrots good for flavor, but they add a nice color to this pasta that could be the base for any number of pasta dishes.
 Carrot Ginger Layer Cake with Orange Cream Cheese Frosting – Most carrot cakes have no frosting or a traditional cream cheese frosting. The idea of an orange frosting makes this cake special.
Carrot Ginger Layer Cake with Orange Cream Cheese Frosting – Most carrot cakes have no frosting or a traditional cream cheese frosting. The idea of an orange frosting makes this cake special.
 Carrot, Ginger, and Lime Juice – Refreshing and healthy.
Carrot, Ginger, and Lime Juice – Refreshing and healthy.
10/22/15
 Susan DeRemer, CFRE
Susan DeRemer, CFRE
Vice President of Development
Discovery Eye Foundation