5/8/14
Charles Bonnet Syndrome
“Do you ever see anything you know is not there but looks real anyway?” I asked Sam Weinberg when he came to the Low Vision Living program.
“No.” he said, looking at his wife, Rachel, and fidgeting with his sweater.
“Oh”, I said casually, “I just asked because many people with macular degeneration see things they know are not there. I call it phantom vision, but the technical term is Charles Bonnet Syndrome.”
“Is this syndrome an early sign of Alzheimer’s?” Sam asked pointedly, still looking at Rachel. . .
“Absolutely not”, I said firmly. “Charles Bonnet Syndrome has nothing to do with mental agility or stability. When you have phantom vision, your mind is fine; it is your eyes that are playing tricks on you. It’s a side effect of low vision.”
“Well,” Sam admitted quickly, “I see little monkeys with red hats and blue coats playing in the front yard. I’ve seem them for eighteen months.”
“What!” Rachel’s eyes about popped out of her head. “Little monkeys in the front yard?”
“Well. . .um,” Sam continued, “sometimes I see them in the living room too.”
What is Charles Bonnet Syndrome (CBS)?
Charles Bonnet was an eighteenth century Swiss naturalist and philosopher. . . who described his grandfather’s curious experience of seeing men, women, birds and buildings that he knew were not there. Later in his life, Bonnet’s own vision deteriorated and he experienced phantom visions similar to his grandfather’s. . . .Charles Bonnet’s discovery didn’t capture medical attention at the time. But 150 years later, in the 1930’s, his files were dusted off, and he was credited with being the first person to describe the syndrome that came to be named for him.
How common is CBS?
This syndrome is very common. Studies place the number somewhere between 10 and 40 percent of people with low vision. Twenty percent of my low vision patients have Charles Bonnet Syndrome. . . To determine whether or not you are experiencing phantom vision: Do the images that appear to you have the following six characteristics?
- They occur when you are fully conscious and wide awake, often during broad daylight
- They do not deceive you; you are aware that they are not real.
- They occur in combination with normal perception. For example, you may see a sidewalk clearly but find it covered with dots, flowers, or faces.
- They are exclusively visual and do not appear in combination with any sounds or bizarre sensations.
- They appear and disappear without obvious cause.
- They are amusing or annoying but not grotesque.

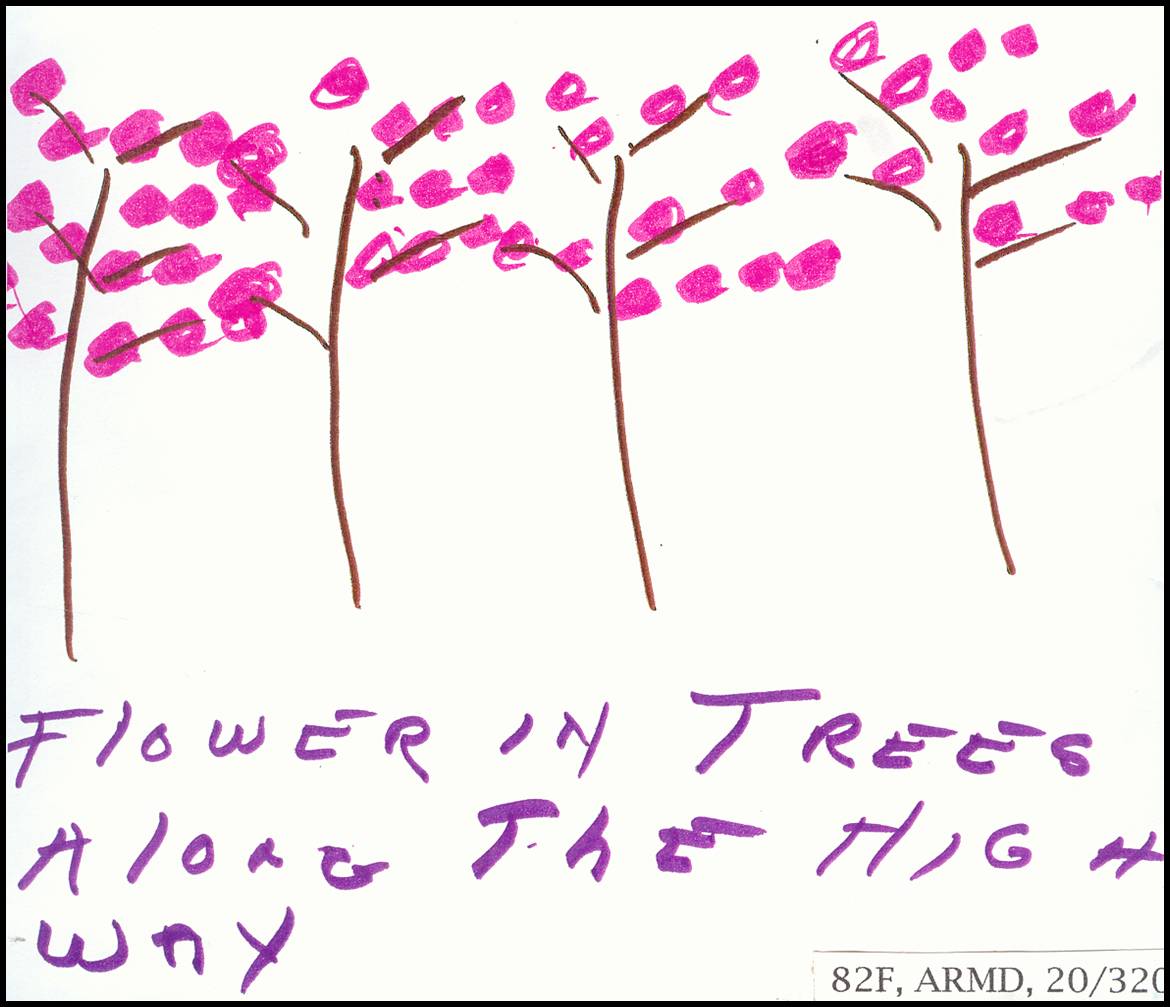
What do people with CBS see?
My patients. . . have reported seeing cartoon characters, flowers in the bathroom sink, hands rubbing each other, waterfalls and mountains, tigers, maple trees in vibrant autumn foliage, yellow polka dots, row houses, a dinner party and brightly colored balloons. . . One of the most remarkable qualities of these figures is that they almost always wear pleasant expressions. . . Menacing behavior, grotesque shapes and scenes of violent conflict are not, to my knowledge, a part of this syndrome.
Usually the same image or set of images reappears to each person. Sam’s monkeys usually materialized around sunset. . .They stayed for 10 or 20 minutes several times a week for two years and then began to appear less frequently. Some times the images change of multiple images appear. . .
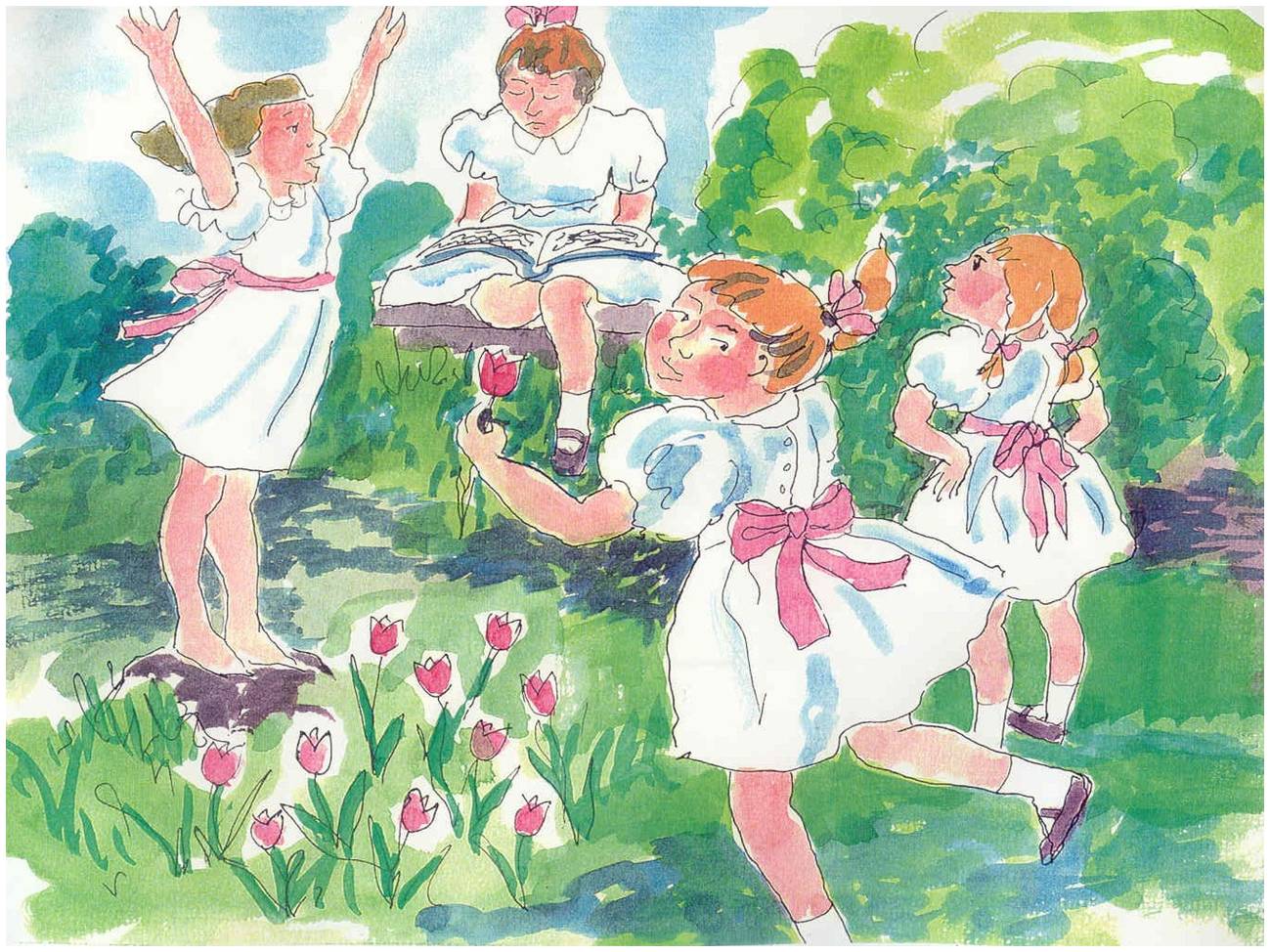
Dolly Kowalski’s Little Girls with Pink Bows
‘I see little girls with pink bows playing in my yard. At first, there was only one little girl. But after a while, she had several playmates. Now they come almost every evening for fifteen minutes. . .They are so delightful, so cheerful, so active. Their little white dresses and pink bows blow in the wind. I see them so incredibly clearly, much more clearly than I see anything else now. . . .I know they aren’t real, but you wouldn’t believe how realistic they seem. . . . I wish you could see them the way I do.’”
Further note by Lylas Mogk, MD
Fortunately, most people, like Dolly, find the images of CBS largely untroubling and many actually find them amusing or enjoyable, as they are usually pleasant and they are crystal clear. There is no drug treatment for CBS, but it is associated with sensory deprivation, so the more active and engaged one is the less likely it is to occur. That’s one reason why vision rehabilitation to empower individuals to accomplish their daily activities in spite of vision loss.
Excerpts were used from Macular Degeneration: The Complete Guide to Saving and Maximizing Your Sight, by Lylas G. Mogk, MD and Marja Mogk, PhD, New York: Ballantine Books, 2003, Chapter 8, pp. 236-252.
![Mogk_Lylas_11C[1]](https://discoveryeye.org/wp-content/uploads/Mogk_Lylas_11C1.jpg) Lylas G. Mogk, MD
Lylas G. Mogk, MD
Director, Center for Vision Rehabilitation and Research
Henry Ford Health System