
4/10/14
During a trip to the optometrist or ophthalmologist, a patient will encounter the process of subjective refraction. This technique involves the clinician asking the patient to make a series of judgments (which is better, one or two?) about the clarity of their vision when looking through a series of lenses. The choices that the patient makes guide the clinician in identifying an optical prescription which is typically made up of sphere, and potentially, cylinder lenses.
Why is it that glasses don’t always work for patients with keratoconus?
In many instances, individuals with keratoconus do not achieve excellent visual performance with spectacles or traditional soft contact lenses. One cause for the failure of these corrections is that the changes in corneal shape that accompany keratoconus induce refractive errors which traditional spectacles simply cannot correct. So, even when sphere and cylinder in the keratoconic eye are well-corrected, these “other refractive errors” or “other aberrations” remain uncorrected and can lead to a blurred retinal image and blurred vision. Collectively these other aberrations can be referred to as higher order aberration, while the aberrations that are typically corrected with spectacles and soft contact lenses are referred to as lower order aberration.
What kinds of higher order aberrations are present in keratoconus:
Pantanelli et al. have stated that the level of higher order aberration present in an eye with keratoconus is, on average, approximately 5.5 times higher than the level experienced in a control group. In an effort to visualize higher-order aberration data, they are commonly represented graphically as shown in the figures below. Examples of higher order aberration measured in one normal eye are shown in figure A, while an example of higher order aberration from one keratoconic eye are shown in figure B. The circular nature of the map denotes the boundary of the measurement, which is defined by the round pupil of the eye. A majority of the higher order aberration map in figure A is green (denoting a relative absence of higher order aberration). However, the map in figure B displays a much larger variation in color, indicating the presence of higher order aberration in this individual keratoconic eye in a greater quantity than the normal eye shown in figure A.
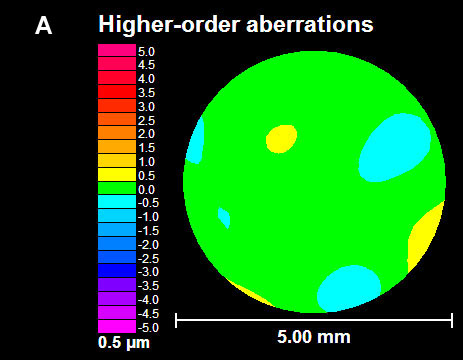
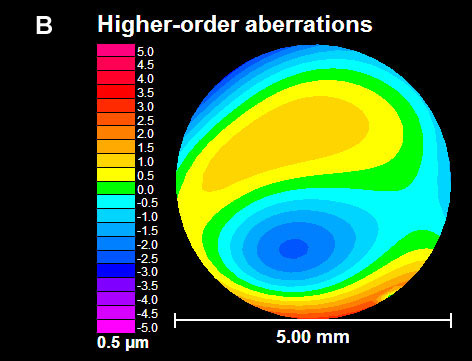
A wavefront aberration map of the “other aberrations” or higher order aberrations of two eyes. Figure A is an example of data for a normal eye and figure B is an example of data for an eye with keratoconus.
If refraction is not capable of quantifying higher order aberrations, how are they measured?
One method for obtaining the information regarding higher order aberration shown above is with a wavefront sensor. The wavefront sensor objectively (without patient feedback) collects information on the optical performance of the eye that can be used to calculate the amount of both lower and higher order aberration present.
Laboratory-based research related to custom contact lenses:
Several investigators in the laboratory (e.g. Katsoulos et al., Sabesan et al., Chen et al., Marsack et al.) have reported on work that attempts to further reduce higher order aberration by targeting the eye-specific higher order aberration seen in a given keratoconic eye. The general philosophy behind these customized lenses is that the aberration pattern measured with the wavefront sensor is a more complete optical prescription for implementation of a custom contact lens. Figure C demonstrates, in principle, the optical properties of a contact lens designed to correct the higher-order aberration in figure B. Where the map of the eye (figure B) is red, the map of the correction (figure C) is blue, and vice versa. When the lens is worn, the net effect as light propagates through the lens-eye system is the cancellation of the higher order aberration in a targeted manner.
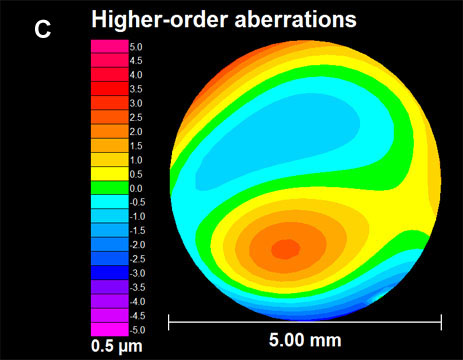
In principle, this figure pictorially represents the higher order optical properties of a contact lens designed to fully correct the higher-order aberration of the eye represented in figure B.
What is next:
Investigators continue to push the technology behind custom contact lenses for keratoconus towards clinical relevance. However, like every novel intervention strategy, we must manage our expectations. Complexity in measuring keratoconic eyes, a need for specialized equipment and expertise to design and manufacture the lenses, the infrastructure needed to coordinate the clinical exam and manufacture efforts and cost associated with the process are a subset of the barriers that must be removed if this type of correction is to become more mainstream. For this reason, it is my opinion that if/when these corrections become commonly available in the clinic, they will likely add to, and not replace, existing forms of corrections that patients and clinicians now utilize to correct vision.
 Jason Marsack, PhD
Jason Marsack, PhD
Research Assistant Professor
University of Houston, College of Optometry.
Dr. Marsack’s work focuses on the relationship between visual performance
and optical aberration in individuals with highly aberrated eyes.