During the height of summer sunshine (and heat!), it’s helpful to discuss the importance of eye protection, including ways to reduce the harmful effects of sun glare.
Fundamentally, we need light to see. Approximately 80% of all information we take in is received through the sense of sight. However, too much light – and the wrong kind of light – can create glare, which can affect our ability to take in information, analyze it, and make sense of our surroundings.
Facts about Sunlight
Every type of light has advantages and disadvantages, and sunlight is no exception:
Advantages:
• Sunlight is the best, most natural light for most daily living needs.
• Sunlight is continuous and full-spectrum: the sun’s energy at all wavelengths is equal and it contains all wavelengths of light (explained below).
Disadvantages:
• It is difficult to control the brightness and intensity of sunlight.
• Sunlight can create glare, which can be problematic for many people who have low vision.
• Sunlight is not always consistent or reliable, such as on cloudy or overcast days.
Visible Light and Light Rays
An important factor to consider is the measurement of visible light and light rays, beginning with the definition of a nanometer:
• A nanometer (nm) is the measurement of a wavelength of light.
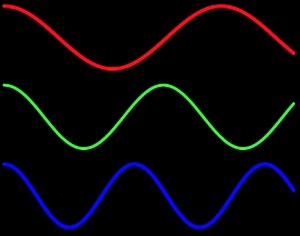
• A wavelength is the distance between two successive wave crests or troughs:
• A nanometer = 1/1,000,000,000 of a meter, or one-billionth of a meter. It’s very small!
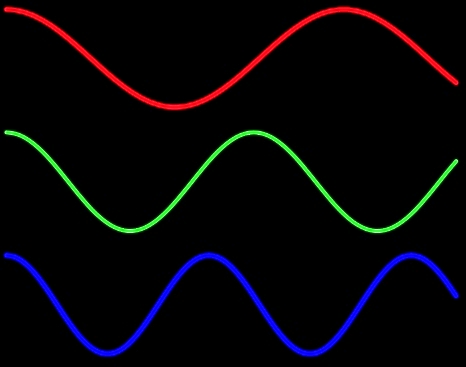
The human visual system is not uniformly sensitive to all light rays. Visible light rays range from 400 nm (shorter, higher-energy wavelengths) ? 700 nm (longer, lower-energy wavelengths).

The visible light spectrum occupies just one portion of the electromagnetic spectrum, however:
• Below blue-violet (400 nm and below), is ultraviolet (UV) light.
• Above red (700 nm and above), is infrared (IR) light.
• Neither UV nor IR light is visible to the human eye.
Ultraviolet Light and Blue Light
Ultraviolet (UV) light has several components:
• Ultraviolet A, or UVA (320 nm to 400 nm): UVA rays age us.
• Ultraviolet B, or UVB (290 nm to 320 nm): UVB rays burn us.
• Ultraviolet C, or UVC (100 nm to 290 nm): UVC rays are filtered by the atmosphere before they reach us.
Blue light rays (400 nm to 470 nm) are adjacent to the invisible band of UV light rays:
• There is increasing evidence that blue light is harmful to the eye and can amplify damage to retinal cells.
• You can read more about the effects of blue light at Artificial Lighting and the Blue Light Hazard at Prevent Blindness.
A new study from the National Eye Institute confirms that sunlight can increase the risk of cataracts and establishes a link between ultraviolet (UV) rays and oxidative stress, the harmful chemical reactions that occur when cells consume oxygen and other fuels to produce energy.
Sunlight and Glare
Glare is light that does not help to create a clear image on the retina; instead, it has an adverse effect on visual comfort and clarity. Glare is sunlight that hinders instead of helps. There are two primary types of glare.
Disability glare
• Disability (or veiling) glare is sunlight that interferes with the clarity of a visual image and reduces contrast.
• Sources of disability glare include reflective surfaces (chrome fixtures, computer monitors, highly polished floors) and windows that are not covered with curtains or shades.
Discomfort glare
• Discomfort glare is sunlight that causes headaches and eye pain. It does not interfere with the clarity of a visual image.
• Sources of disability glare include the morning and evening positions of the sun; snow and ice; and large bodies of water, (including swimming pools).
Controlling Glare
You can protect your eyes from harmful sunlight and minimize the effects of glare by using a brimmed hat or visor in combination with absorptive lenses.
• Absorptive lenses are sunglasses that filter out ultraviolet and infrared light, reduce glare, and increase contrast. They are recommended for people who have low vision and are also helpful for people with regular vision.
• Lens colors include yellow, pink, plum, amber, green, gray, and brown. Ultra-dark lenses are not the only choice for sun protection.
• Lens tints in yellow or amber are recommended for controlling blue light.
• NoIR Medical Technologies: NoIR (No Infra-Red) filters absorb UVA/UVB radiation and also offer IR light protection.
• Solar Shields: Solar Shields absorb UVA/UVB radiation and are available in prescription lenses.
• You can find absorptive lenses at a specialty products store, an “aids and appliances store” at an agency for the visually impaired, or a low vision practice in your area. Before you purchase, it’s always best to try on several different tints and styles to determine what works best for you.
More Recommendations
• Always wear sunglasses outside, and make sure they conform to current UVA/UVB standards.
• Be aware that UV and blue light are still present even when it is cloudy or overcast.
• Make sure that children and older family members are always protected with UVA/UVB-blocking sunglasses and brimmed hats or visors.
 Maureen A. Duffy, CVRT
Maureen A. Duffy, CVRT
Social Media Specialist, visionaware.org
Associate Editor, Journal of Visual Impairment & Blindness
Adjunct Faculty, Salus University/College of Education and Rehabilitation

 My supervisor said not to work so hard to explain. He thought it was a nonissue: “If you were blonde and blue-eyed, would you be describing that over the phone to them?” he asked. He was right. It didn’t faze most people. In the 11 years I’ve been practicing, only a few people had a problem with it. To this day, once in a while, it may come out organically that I’m blind. Most of the time, I don’t tell them beforehand.
My supervisor said not to work so hard to explain. He thought it was a nonissue: “If you were blonde and blue-eyed, would you be describing that over the phone to them?” he asked. He was right. It didn’t faze most people. In the 11 years I’ve been practicing, only a few people had a problem with it. To this day, once in a while, it may come out organically that I’m blind. Most of the time, I don’t tell them beforehand. Kooshay Malek
Kooshay Malek