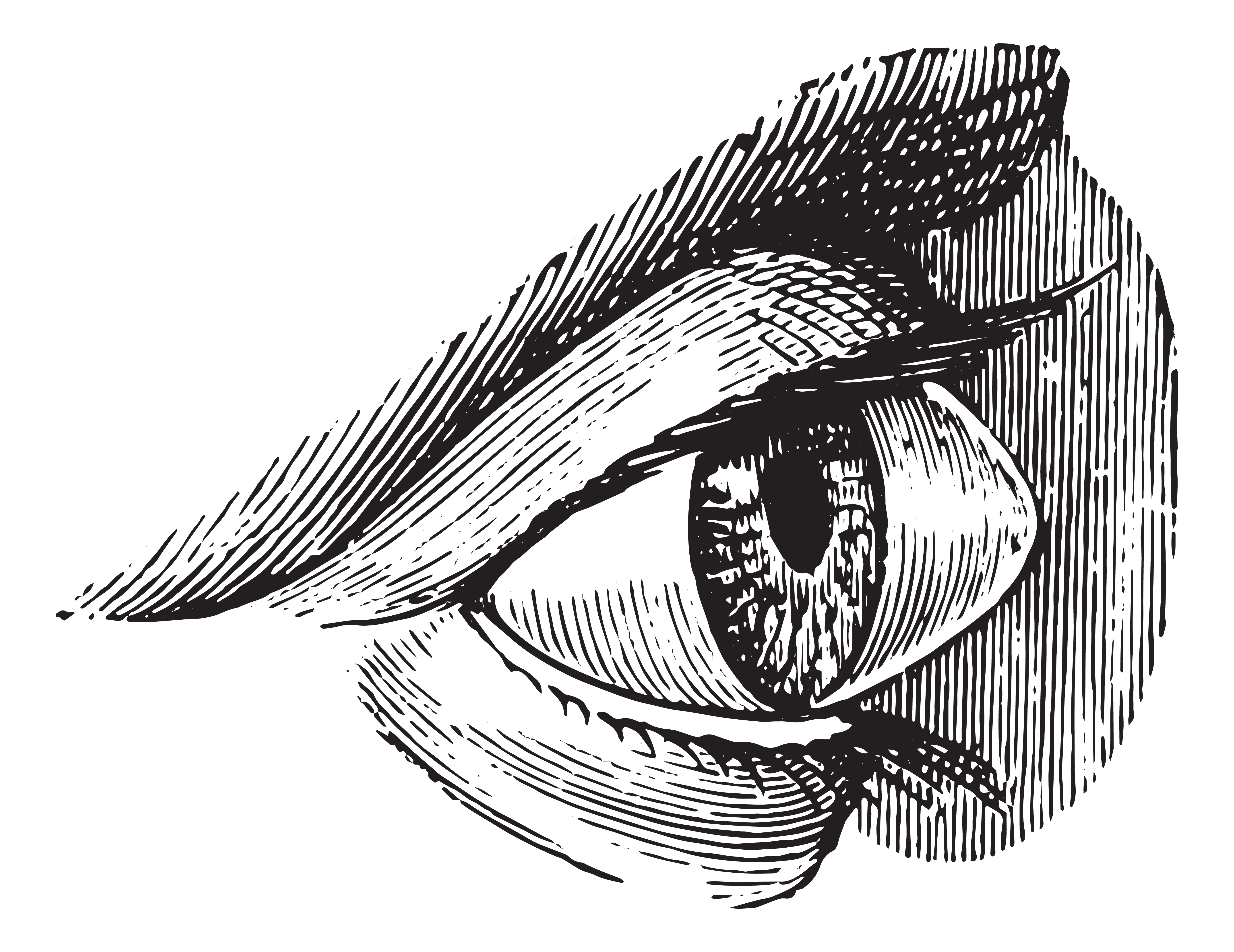
A pterygium (pronounced tur-IJ-ee-um) is a wing-shaped, fleshy growth of tissue that grows from the conjunctiva (the clear thin covering of the sclera or white part of the eye) onto the cornea (the clear front of the eye). The word pterygium comes from the Greek, pterygos, which means little wing. Pterygia are quite common and can be seen in surfers (hence the common reference as surfer’s eye), sunbathers, landscape architects and other outdoor people who do not adequately protect their eyes from the damaging ultraviolet radiation from the sun. Furthermore, people living closer to the equator have been shown to have a higher incidence of pterygia. Prolonged exposure to eye irritants such as wind and dust are also risk factors for the development of pterygia.
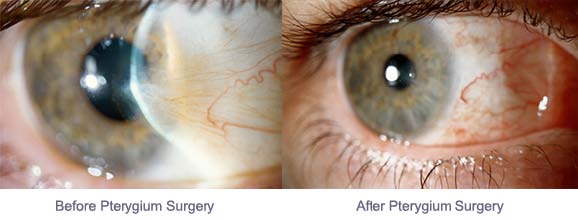
Pterygia usually grow slowly or follow an indolent course and can be asymptomatic or can flare up from irritation. Early on, pterygia may not be even noticed and may not be serious. Or, there can be signs of dry eyes, such as mild burning, tearing and itching due to irregular tear wetting of the surface of the eye. As the pterygium grows in size, the lesion will become more noticeable and may become cosmetically unpleasant, irritating to the patient and may give the sensation of a foreign body in the eye. Pterygia may cause visual symptoms if they induce astigmatism as they approach the center of the cornea or visual axis. Once the pterygium grows towards the visual axis, where vision could be compromised, various surgical procedures can be employed to remove it.
Having an ophthalmologist (an eye MD) examine your eyes is the first step to making the correct diagnosis and receiving the appropriate treatment, if it is necessary. Your ophthalmologist will examine the front of your eyes with a slit lamp, a specialized microscope for eye examination. Early in the disease process, most ophthalmologists will take a conservative approach and treat with lubricating eye drops and recommend protective eye wear (to prevent further UV exposure) and use of a wide-brimmed hat. If the pterygium enlarges and grows onto the cornea towards the visual axis, the ophthalmologist will consider surgical intervention to halt any more damage and scarring to the eye. Sometimes, a more aggressive pterygium may induce astigmatism on the cornea (causing the cornea to become more oval or football-like in shape as compared to more round in shape like a basketball). Astigmatism may cause blurred vision and, if left untreated, may not be reversed even with surgical intervention. Long-lasting pterygia may cause irreversible scarring of the underlying cornea, which may leave the cornea with a thin white film, or scar, even after the removal of the pterygium. If this scar is out of the visual axis, then vision may not be affected.
There are several different surgical techniques that are commonly used to remove aggressive pterygia. Microsurgical techniques can be done safely and comfortably on an outpatient basis in an eye surgery center using local anesthesia with mild sedation. The most common surgical technique involves surgical removal of the pterygium, placement of a preserved amniotic membrane graft (from the placenta) or a small graft of the patient’s own conjunctiva taken from the superior (upper) part of the conjunctiva to cover the area where the pterygium was removed, and using fibrin glue and/or small sutures to hold the graft in position. This procedure usually takes 30 minutes to one hour to perform, depending its complexity, with little discomfort for the patient. Post-operatively, the patient usually wears a patch for one day and can return to work after a few days (avoiding eye rubbing, swimming and hot tubs). Topical antibiotic and steroid drops and/or ointments are used for several weeks or months on a tapering dosage schedule per your ophthalmologist. Steroid medications reduce inflammation and chance of recurrence and should be used as directed. Careful follow-up for a year after surgery is recommended.
The main risk of pterygium surgery is recurrence of the pterygium after removal with a regrowth of abnormal tissue onto the cornea. When an amniotic membrane graft or conjunctival auto-graft is not used, the recurrence rate is quite high and has been reported from 25% to over 50%. However, when these grafts are used, the recurrence rate can be as low as 5 to 10%. For recurrent pterygium removal, however, the recurrence rate can be much higher and other adjunctive therapy may be utilized. Intraoperative mitomycin C (MMC) is often used in addition for recurrent pterygium excision to inhibit the regrowth of the pterygium. Some ophthalmologists use MMC eye drops after excision. Discuss these options with your ophthalmologist before your surgery. Be sure to see your ophthalmologist if you have a pterygium so that it can be properly assessed and appropriate treatment can be performed.
3/19/15
 Ronald N. Gaster, MD, FACS
Ronald N. Gaster, MD, FACS
Gaster Eye Center
Beverly Hills and Huntington Beach, CA