The term “vision rehabilitation” covers a wide range of services that can help you learn how to remain active with vision loss while maintaining your independence and quality of life.
Vision Rehabilitation Services
The following are different vision rehabilitation services you can access in addition to the information and help you will receive from your ophthalmologist or optometrist.
Communication skills: These help you with reading, writing and assistive computer technology. In some cases you may even want to learn braille.
Counseling: This can be beneficial, not only to you, but and family and/or friends that want to better understand or help you with your vision loss.
Independent living skills: These skills can be a simple as learning how to cook safely, take care of your personal appearance, manage your finances, keep exercising, or enjoy hobbies. The people that come to your home to help you keep your independent may also suggest home modifications to make life easier and help ensure your safety.
Independent movement and travel skills: These skills are important not only to help with your independence, but also to keep you from isolating yourself. Isolation is a common problem with vision loss as you may not want people to know you are losing your vision, or you are afraid of falling or embarrassing yourself. However, isolation can lead to depression.
Low vision evaluations and training: There are a variety of hand-held and desktop magnifiers, special reading glasses, lighting sources and other devices that help you make the most of your remaining vision.
Vocational rehabilitation: Loss of vision does not necessarily mean you can no longer work. Vocational evaluation and training, along with job modification and restructuring, can keep you enjoying the work you have enjoyed and depend on.
Vision Rehabilitation Service Providers
When looking for vision rehabilitation services, what should you know? You are best looking for a specially trained person including low vision therapists, vision rehabilitation therapists, and orientation and mobility specialists. They each have completed a standardized certification process that will let them help guide you as you work toward your vision goals.
Certified Low Vision Therapists (CLVTs): These therapists work with you to use your remaining vision with various devices and assistive technology. They also help you determine what modification you might need at home or work to remain independent and safe.
Certified Vision Rehabilitation Therapists (CVRTs): These therapists teach special adaptive skills that will allow you to confidently carry out a range of daily activities.
Certified Orientation and Mobility Specialists (COMS or O&Ms): These specialists teach skills that help you navigate safely and confidently when you are home, in the community or traveling far from home. This can include the use of a cane, GPS devices or public transportation. They also include guide dog instructors, but this training is more intense and takes place at a guide dog facility for several days.
To remain active and independent may require learning new skills, but it is important to find the right person to help you learn those skills. By finding the best person to suit your needs, the process can be a fun and positive experience.
The introduction of the excimer laser to eye surgery in the early 1990’s represented a revolutionary innovation in the treatment of refractive errors: nearsightedness, farsightedness, and astigmatism. The development of this technology allows the safe and dependable correction of vision in many patients. For the most part, however, keratoconus (KC) patients are not candidates for such procedures for 2 reasons. First, the inherent biomechanical weakness of the keratoconic cornea could worsen if tissue is removed from the already thin cornea. Second, in addition to standard nearsightedness, farsightedness, and astigmatism, keratoconic vision is also impeded by higher order aberrations, which can be thought of as static in the eye’s optical system. However, recent advances may make variations of such procedures applicable to selected patients with KC.
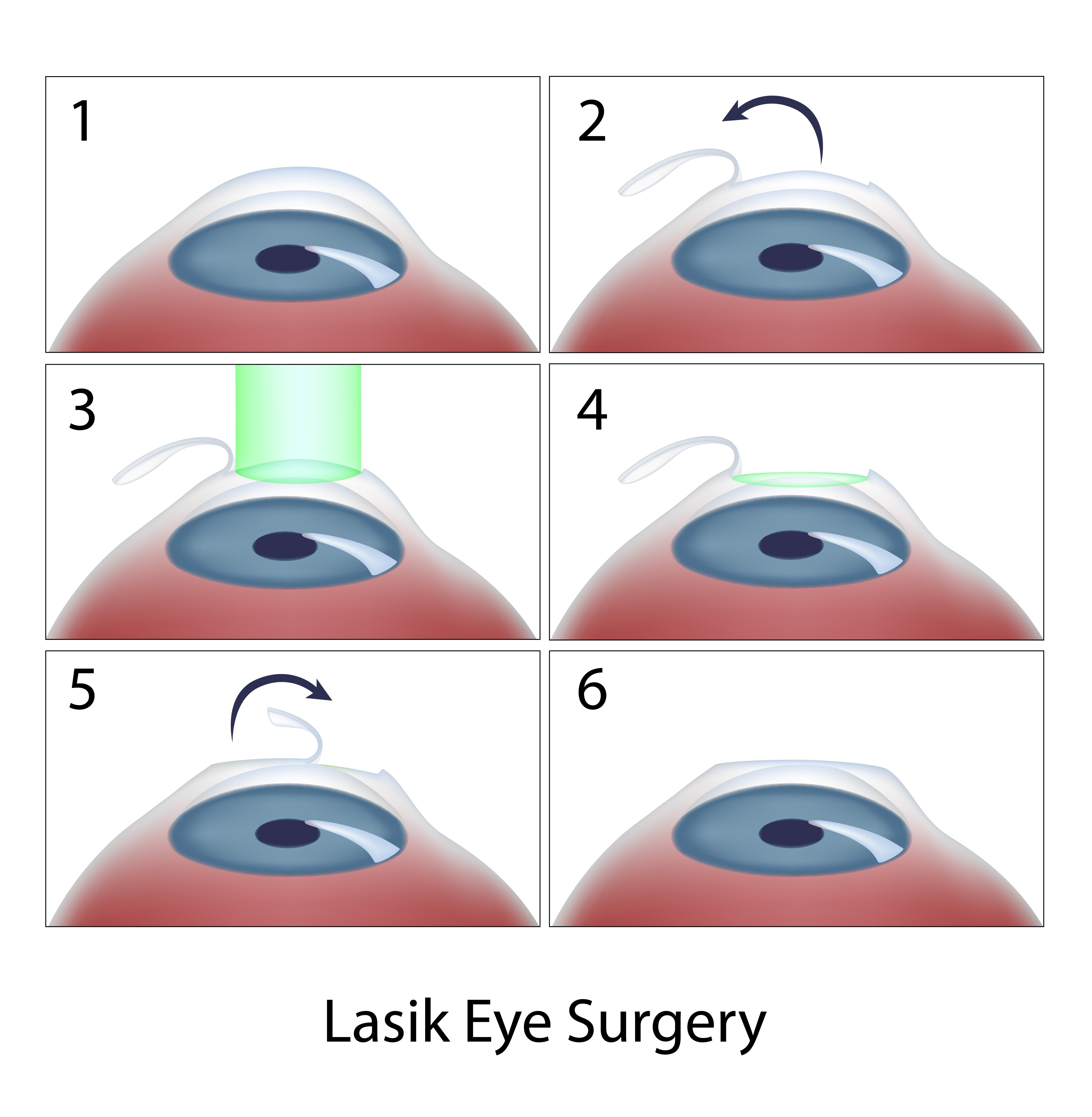
LASIK, LASEK, PRK and PTK
Today, laser in situ keratomileusis (LASIK) is the most popular method of laser eye surgery. LASIK uses an excimer laser to correct nearsightedness, farsightedness, or astigmatism by removing a thin lenslet of tissue from the surface of the cornea (the clear, front “watch crystal” of the eye). This is analogous to removal of a “tissue contact lens”. In LASIK, which is now an “all-laser” technique, a pancake-like thin flap of the cornea is first prepared with a high speed femtosecond laser. The flap acts to preserve the surface epithelial cells (which are like tiles on a floor) to promote quick healing and recovery of vision. Next, the excimer laser is used to remove a small amount of tissue from the corneal surface beneath the flap. The excimer laser used in LASIK produces a beam of invisible ultraviolet light energy, which when applied via an eye tracking mechanism, results in meticulous removal of this “tissue contact lens”. After corneal reshaping, the LASIK procedure is finished when the corneal flap is repositioned. When the flap is replaced, it lies in the bed of excimer laser removed tissue, causing the surface to change shape with the effect of decreasing nearsightedness, farsightedness, or astigmatism.
Laser vision correction can also be performed without a LASIK flap. These procedures, which are also perfomed with the excimer laser, go by a number of names – PRK (photorefractive keratectomy), LASEK (laser epithelial keratomileusis), epi-LASIK, or ASA (Advanced Surface Ablation). Although LASEK and LASIK sound the same, unlike traditional LASIK, LASEK does not require the preparation of a corneal flap. This has two potential advantages. First, risks of making the corneal flap in LASIK are avoided. This may be important in some patients in whom there is an additional risk in making the flap, such as patients with corneal scars or irregularities. Second, since laser treatment is done on the surface, LASEK/PRK preserves more corneal tissue. In particular, patients who have thinner corneas may be more safely treated with a no flap technique rather than LASIK.
At the beginning of the LASEK / PRK eye surgery procedure, the surface cells of the cornea are loosened and removed. The laser treatment then is applied, just as in LASIK, removing the properly shaped “tissue contact lens” for the desired optical correction. At the end of the procedure, a contact lens bandage is applied. Topical drops are used for a few week afterwards to avoid infection and control wound healing.
Vision after LASEK/PRK takes a little while longer to completely improve and stabilize than after LASIK because the epithelium needs to grow and smooth. Substantial improvement usually is noticed the day after the procedure and fluctuates over the next 2 weeks. The contact lens is removed in 5 days in most patients. Driving vision in the days after the procedure can be variable and take up to 2 weeks in some patients.
For both LASIK and LASEK/PRK, there are two basic types of possible side effects. Because patients may respond and heal differently, it is possible that the entire refractive error may not be fully corrected. In this case, vision will be clearer without glasses, but may not be as good as desired. In these situations, patient often can undergo a re-treatment procedure to further improve their vision. In addition, optical side effects include halos around lights and glare, especially at night, and some patients may experience dry eye sensations. Other, more rare, complications include infection or scarring.
Recently, there has been much talk in the keratoconus community about combining corneal collagen crosslinking with topography-guided LASEK/PRK. Topography-guided PRK uses information gained from your corneal map to program the laser to help make your cornea more optically regular. The goal of topography-guided PRK, like Intacs, is to improve corneal contour in the KC patient to improve glasses corrected vision and contact lens tolerance. In general, you will still need contacts and glasses afterwards.
Typically, LASEK/PRK procedures for keratoconus are combined with corneal collagen crosslinking, which has the goal to strengthen the weak keratoconic cornea and decrease progression of corneal mishapening over time. It is important to note that such treatments are not FDA-approved and are not generally available in the U.S. However, a number of international surgeons have been exploring the potential role of combined LASEK/PRK with crosslinking to improve keratoconus outcomes. In our practice, we have also had the opportunity to use Intacs and other procedures to further improve corneal shape in patients who have undergone topography-guided treatments with crosslinking with encouraging results.
In addition to LASIK and LASEK/PRK, the excimer laser may provide a novel therapeutic modality in the treatment of a number of superficial corneal disorders. This treatment is known a phototherapeutic keratectomy or PTK. Whether PTK eye surgery is used alone or as an adjunctive strategy in traditional corneal surgical techniques, a number of disorders affecting the corneal surface may be successfully treated by taking advantage of the excimer laser’s ability to meticulously remove superficial corneal tissue. These include a variety of corneal degenerations and dystrophies, corneal irregularities, and superficial scars, such as surface nodules found at the apex of the keratoconic cone. While some of these conditions, heretofore, could be treated by mechanical superficial keratectomy techniques, PTK may minimize tissue removal and surgical trauma.
So, for patients with keratoconus, it is important to know that, although LASIK type procedures are generally not indicated, research using these advanced technologies continues. A tailored therapeutic approach over time may combine a variety of procedures to optimize the corneal shape and ultimate visual outcome for the patient with keratoconus.
9/15/15
Peter S. Hersh, MD
Cornea and Laser Eye Institute – Hersh Vision Group
CLEI Center for Keratoconus
Adults and children do not learn in the same way. The concept of “andragogy” was widely introduced to the world of educational theory by Malcolm Knowles, PhD, in the latter part of the 20th century. He contrasted “pedagogy,” which is generally used to describe the method or practice of teaching — and comes from the Greek for “child learning” — with the practice of “andragogy,” which applies specifically to adult learning. While Knowles did not invent the term, he advanced the argument that andragogy should be very different from pedagogy.
Maureen Duffy, CVRT, LVT, an editor for Journal of Visual Impairment & Blindness, a writer and blog editor for VisionAware, and author of Making Life More Livable: Simple Adaptations for Living at Home After Vision Loss, relies heavily on andragogy in her work with vision-impaired adults. Loved ones — especially adult children of older people — have a tendency to push care and “help” on grown-ups as if they were children, she says. Not surprisingly, this method seldom works.
Using Andragogy to Help People with AMD
From her work as a certified vision-rehabilitation therapist (CVRT) and low-vision therapist (LVT), Duffy calls out three concepts of andragogy to keep in mind when trying to help an adult who is coping with vision loss:
1. Adults have life experience.
Children don’t have a lot of life experience. And while adults have an incredible amount of life experience, we don’t always treat them as if they do. They already know how to problem-solve. If they have been cooking for their entire lives, they don’t need to learn to learn how to cook all over again; they just need to make adaptations.
“We treat adults as if they have to forget everything they’ve learned, and try to teach them something new,” Duffy says. “That doesn’t usually work. I say, ‘Show me how you’ve always done this. There’s probably just a little adaptation you need to make, and you can keep doing things the way you’ve always done them.’ You can’t just go in, and tell someone you’re going to change everything they do. Just figure out an adaptation.”
2. Adults are reactive learners.
Children are ready to learn when they are told they are ready to learn: We send them to school, and they know it’s time to learn. Adults are ready to learn when they decide they need to know or do something to improve their daily lives — not before. You cannot make an adult learn until they are ready to learn. That’s a big difference.
“Adults tend not to say, ‘I’m going to learn this now because I might need it later.’ They say, ‘I have this problem right now; I need to learn this thing right now,’” Duffy says. “It’s common for family members to tell a person with macular degeneration, ‘You need to learn braille in preparation for when you go blind in the future.’ That’s not true. They can read larger and larger print for as long as they are able to do so. It creates additional anxiety to tell an adult they have to start now to prepare for when they can’t see. You can’t prepare for that. It’s a process, and you make changes as you go.”
3. Adults are self-directed.
Adults want to be independent and determine, for themselves, what it is they need to learn. And that won’t necessarily match what family members think or want.
“Adults will decide what they want to learn, usually based on a hierarchy of needs and what they really need to know now,” Duffy says. “That hierarchy starts with survival needs: making food, getting food, reading medications, etc. And the only way to know what an adult wants and needs to learn is to ask them.”
At the heart of andragogy, it seems, is respect for the fact that an adult is an adult — and should be treated as such. “Andragogy is more focused on teaching problem-solving skills, which can be used over and over again by the adult in a variety of situations,” Duffy says.
Another difference between the way children and adults learn is the need for adults to maintain a sense of autonomy, points out Judi Delgado, director of the Macular Degeneration Partnership (MDP). “People with AMD may need to adjust the way they do some things, but they can still do them,” she says. “It doesn’t help them if others try to take over or do things for them. It’s important to understand that the person is already losing so much; if loved ones try to take over their lives, it just adds to the loss of independence.”
9/10/15
Maureen A. Duffy, CVRT, LVT
Social Media Specialist, visionaware.org
Associate Editor, Journal of Visual Impairment & Blindness
Adjunct Faculty, Salus University/College of Education and Rehabilitation
Receiving a diagnosis of age-related macular degeneration (AMD), diabetic retinopathy or glaucoma can be a shock. Loved ones naturally want to help, but they don’t always know what to do or how to do it. Here are 3 tips for caregivers helping people with low vision.
We asked vision-rehabilitation expert Maureen Duffy, CVRT, for advice. She suggests turning to local low-vision agencies, trained low-vision professionals and online resources, such as the Macular Degeneration Partnership and the VisionAware services guide. Perhaps most importantly, she says, look for a support group.
“I have found that most adults with whom I’ve worked turn to their peers, and they get the most guidance and help in vision-loss support groups,” says Duffy, an editor for Journal of Visual Impairment & Blindness, a writer and blog editor for VisionAware, and author of Making Life More Livable: Simple Adaptations for Living at Home After Vision Loss.
Duffy shared the three most important things to ask a loved one after they find out they have AMD:
1. What do you understand about what the doctor said and about what’s going on with your vision? What don’t you understand? What do we need to clear up?
If they don’t understand completely, ask if you can go to doctor with them to be a note-taker and information-gatherer. Ask the doctor for explanations. Be clear and concrete about the information you need — and ask the doctor for next steps.
The Macular Degeneration Partnership website has a downloadable list of questions to take along, as well as suggestions on how to be an advocate during a visit to the doctor on its “Be an Advocate” page.
2. What is the one thing you are most afraid of RIGHT NOW?
At first, their biggest fear is of going totally blind: “I won’t be able to do anything; I’ll be all alone; I’ll be totally helpless.” With AMD, they won’t go totally blind, and they can learn to make the most of their peripheral vision. There are services that can help, but it’s tough in the beginning: Go slowly.
Vision-rehabilitation services can help teach them to function safely and independently in critical day-today activities, such as:
• Independent movement and travel:
getting around indoors
walking with a guide
using a long white cane
crossing streets
using public transportation
using electronic travel devices
• Independent living and personal management:
preparing meals
managing money
labeling medications
making home repairs
enjoying crafts and hobbies
shopping
• Communication and technology:
telling time with an adapted clock or watch
signing their name
using tablets and smartphones
using computers with speech or screen magnification
learning braille
3. What is the ONE thing you are most afraid you can’t do?
Don’t start talking about everything that may need to go on; it’s just too much and is overwhelming. Start with the one thing. “I can’t aim for the toilet”; “I can’t keep food on the fork”; “I can’t make my coffee in the morning.” Help them find solutions for simple things. Figure out alternatives. That little bit of accomplishment encourages self-analysis.
“Many people have difficulty telling currency bills apart,” Duffy says. She shares a simple, effective way to do this by folding each bill differently:
Keep the $1 bill flat and unfolded.
Fold the $5 bill in half crosswise (with the short ends together).
Fold the $10 bill in half lengthwise (with the long sides together).
Fold the $20 bill like a $10 bill lengthwise, and then in half again crosswise, like the $5 bill.
It’s important to remember that no matter how much you may want to help, your loved one may not be ready to accept assistance. Pushing too much too soon isn’t helpful. Once you ascertain that your loved one is ready to be receptive, offer your help gently, slowly and with empathy.
9/8/15
Maureen A. Duffy, CVRT
Social Media Specialist, visionaware.org
Associate Editor, Journal of Visual Impairment & Blindness
Adjunct Faculty, Salus University/College of Education and Rehabilitation
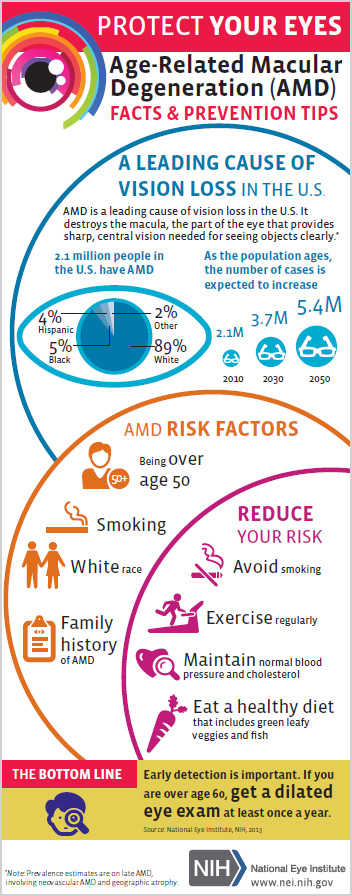
Age-related macular degeneration (AMD) is the leading cause of vision loss in people over 60. And as we continue to live longer, our chances of being affected, either by being diagnosed, or being a caregiver for someone close who is diagnosed, increases considerably. This infographic from the National Eye Institute clearly defines who is at risk, what the risk factors are and how to reduce your risk – what you need to know about AMD.
Cortical Visual Impairment (CVI) refers to decreased vision resulting from the visual processing parts of the brain (e.g., the posterior visual pathways and/or the occipital lobes) rather than from the eyes themselves. For example, individuals with CVI typically have normal eye exam findings. However, vision loss from CVI can range from mild to total blindness. It is also one of the more frequent causes of visual impairment in children. Regardless, children with CVI often have some level of vision that may improve over time, particularly if they receive therapy to teach them how to integrate the visual signals their brains are receiving.
CVI may be caused by a number of different conditions that damage the visual parts of the brain. Examples include stroke, decreased blood supply to the brain, decreased oxygenation in the brain, brain malformation or infection, hydrocephalus, seizure, metabolic diseases, head trauma, and other neurologic disorders. Conditions such as these make it difficult for the brain to understand and interpret what the eyes see.
In most cases, individuals with CVI do not have other neurological problems, although epilepsy and cerebral palsy are not uncommon. The presence of CVI is not an indicator of the cognitive abilities of the individual; therefore, CVI should be distinguished from vision loss secondary to global neurological damage, where other functional deficits are also present in motor, cognitive, and physical abilities.
Indicators of Cortical Vision Loss
In children, one of the most common indicators of CVI is their poor attention to visual targets, particularly to more complex targets, such as a person’s face. Other indicators are that children with CVI often prefer to look at lights for long periods of time and that when reaching for an object, they will often look away from the object before grabbing it. This is because children with CVI have difficulty integrating visual stimuli (looking at an object) with their motor ability (grabbing the object). The diagnosis of CVI is given based on the combined results of magnetic resonance imaging (also known as an MRI) and an eye evaluation by a pediatric ophthalmologist.
Treatments
If a child is suspected of having CVI, he or she should be evaluated by a pediatric ophthalmologist as part of the initial evaluation. The pediatric ophthalmologist will assess the child’s eye health as well as the need for glasses to make sure there are no additional factors that may be limiting vision.
Often, there is concern that a child with CVI has little to no vision early in life. However, vision is a learned sense, so as the child matures, he or she may have improved visual responses. As such, early intervention is important for improved visual responses over time, as well as because the treatment period for visual development is limited to the early years of life. State and local educational agencies and early intervention programs should be contacted as soon as a visual concern is noted so that an organized plan of visual stimulation activities can be developed and implemented, based on the specific needs of each child. The professionals involved in the evaluation of a child with vision loss from CVI can include teachers of students who are blind or visually impaired, physical therapists, occupational therapists, speech therapists, and certified orientation and mobility specialists. It is important to note that although the vision of an individual with CVI may improve with intervention, rarely does the vision become totally normal.
The realization and acceptance that a child is visually impaired can be a difficult adjustment for the child’s parents. Fortunately, there are many things that can enhance the functional abilities of individuals with vision loss at any age. To learn about available resources for individuals with vision loss, visit the National Eye Health Education Program low vision program page.
9/1/15
Mark Wilkinson, OD
University of Iowa Carver College of Medicine
Director, Vision Rehabilitation Service, UI Carver Family Center for Macular Degeneration
Medical Director, UI Optical
Chair of the National Eye Health Education Program Low Vision Subcommittee
Many children who are 6 – 18 years old are now back in school or will be shortly. But have you given them everything they need to succeed in the school year ahead?
? New binders
? Notebook paper and dividers
? Pencil box filled with pens and pencils
? Calculators, protractors and rulers
? Backpack to carry it all
These are the tools that children and their parents focus on every year, thinking these will help their child have a fun and productive year. But the list is incomplete. For school-aged children, the AOA recommends eye exams for children every two years if no vision correction is required. Children who need eyeglasses or contact lenses should be examined annually or according to their eye doctor’s recommendations.
“But my child gets and eye screening at school every year…” While this may be true it is important to understand the difference between a screening and an eye exam.
Vision screenings are a short examination that can indicate a vision problem or a potential vision problem; however it cannot diagnose exactly what is wrong with your eyes. It can also easily miss vision issues, giving parents a false sense of security.
With an eye exam, the tests are performed by a trained professional, using specialized equipment looking for specific indicators that could affect your child’s vision. They test much more than how well your child can read letters or symbols at a distance.
Good vision is necessary for a child to succeed at school and not become frustrated or depressed. It has been estimated that as much as 80% of the learning a child does occurs through his or her eyes. Children need to read a book and see a whiteboard, write and use computers every day in the classroom and at home. When a child cannot see clearly, it becomes more difficult to learn.
It also goes beyond just seeing clearly. Your child needs their eyesight to understand and respond to what they see. This includes the ability to focus their eyes, use both eyes together, and move them effectively.
Children may not always know they have a vision problem because they think that everyone is seeing the way they do. There are some signs that may indicate a vision issue:
Repeated eye rubbing
Excessive blinking
Short attention span
Tilting the head to one side or covering one eye
Holding reading materials too close to the face
Losing their place when reading
Difficulty remembering what they just read
Trying to avoid reading or other close activities
Numerous headaches
So as you prepare your child to go back to school, give them the best advantage they can have – good vision. Make an appointment with your eye doctor today.
This is the third and final installation of the comprehensive series we have presented on dry eye disease. Dr. Wade first discussed the symptoms you might experience if you have dry eye and the Dr. Garg explained the process of diagnosing they type of dry eye disease you might have. In this article Dr. Farid reviews treatment options based on your diagnosis of dry eye disease.
Treatments for Dry Eye Disease
As our understanding of dry eye disease expands, so do treatment options. We now know that dry eye disease is a multifactorial disease. There is no one cause so there is no one magic cure. Treatments aim to improve tear composition, reduce eye surface inflammation, and target eyelid margin disease. Here, we will review many treatment options, but the treatment combination or “cocktail” that is appropriate for you will depend on your specific type of dry eye disease. This is usually determined after some testing by your eye care provider.
Environmental, Dietary, and Medication Adjustments
Before going into specific dry eye treatments, there are modifiable causes and preventative methods to improve dry eyes. Simple changes in the environment, diet, and medications can be easy ways to improve symptoms.
Environmental Changes
As expected, a dry environment will worsen dry eyes. Humidifiers and moisture goggles have been shown to help alleviate these symptoms. Furthermore, situations that cause decreased blinking, such as prolonged use of computer screens, can worsen dry eyes. Patients should take frequent breaks from computer screens and reading, allowing their eyes to rest and resume normal blinking. When in windy, smoky, or dusty situations, sunglasses can act as a barrier to the eyes, reducing dry eye symptoms. Avoiding wind, fans, or any source of air blowing into the eyes may also help.
Dietary Changes
Drinking adequate water keeps patients hydrated and reduces exacerbations of dry eye symptoms. Omega-3 fatty acids, particularly eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), have been shown in many clinical studies to improve dry eyes. It is believed that these fatty acids help inhibit inflammatory mediators. Essential fatty acids cannot be synthesized and must be ingested through diet. Foods rich in omega-3 fatty acids include fish, other seafood, and flaxseed oil. Supplements are also available.
Adjusting Medications
Many medications are associated with dry eyes, and patients may benefit from adjusting doses or finding alternative treatments. You can work with your physician to weigh the costs and benefits about modifying your current medications if they are suspected to worsen dry eyes. Some of these medications include: hypertensive drugs, antihistamines, decongestants, antidepressants, acne medications, birth control, and hormone replacement therapy. Eye drops with preservatives, such as glaucoma medications, can also worsen dry eyes.
Lubricating Treatments
For patients with decreased tear production, supplementation of tears or reduction of tear drainage will improve symptoms.
Artificial tears, gels, and ointments
Artificial tears, gels, and ointments are readily available over the counter. Artificial tears are eye drops that are used throughout the day as needed, up to eight times for dry eyes. You must make sure to get “lubricating” drops. There are multiple available brands that are excellent and equivalent in providing artificial moisture. Avoid “redness relief” brands as they are focused on reducing appearance of the vessels in the eyes as opposed to actual dry eye relief. Gels and ointments are thicker and very effective but can blur vision. Non-commercial comparison testing between brands has not been done. Because the ingredients, preservatives, and consistency vary from brand to brand, it is recommended for patients to choose the best option that works well for them based on trial and error.
Preservatives are used in many eye drops to help them to last longer. Unfortunately, they can be irritating to the eyes, especially when used often (more than 4 drops/day) or with other drops containing preservatives (ie. glaucoma medications). Patients who frequently use eye drops are recommended to use preservative-free (PF) drops. Unfortunately, preservative-free drops are more expensive because they come in “single use” containers. You may be able to extend the life of each single use container by spreading out its contents over multiple uses throughout the day.
Lipid-containing lubricants, such as those with castor oil, attempt to mimic the oils found in the tears, reducing evaporative dry eyes, but more research is necessary to study their efficacy.
Punctal Plugs
Your ophthalmologist can place small plugs at a clinic visit into the punctum, a small hole at the upper and inner lids that drain tears from the eyes. One plug can be added initially, and if more tear retention is required, another plug can be added. There are absorbable and non-absorbable types. Absorbable types are made of collagen and last 1 week to 6 months. Once placed, they are not visible or removable. Non-absorbable plugs are usually silicone, and permanent. They are easily placed by your ophthalmologists and remain visible in follow-up exams. Some patients feel the plugs, and there may be mechanical rubbing, especially when the plug is not the proper size. Some patients may also experience excessive tearing with plugs. If problematic, patients can wait for the plugs to dissolve if absorbable or they can be removed with forceps if non-absorbable.
Autologous Serum
Serum is extracted from a patient’s blood and turned into an eye drop. The growth factors, vitamins, and antibodies present in serum are the same as those in natural tears. Evidence is showing significant promise in alleviating symptoms and signs of chronic dry eye disease. A good collaboration between a phlebotomy lab and compounding pharmacy is necessary to make the products. The products must be kept refrigerated or cold between uses. They can be frozen for long-term storage. Each blood draw provides a supply of drops that can last 3-6 months.
Hydroxypropyl Cellulose Ophthalmic Inserts (Lacrisert)
An insert is available for people who find regular artificial tear use to be difficult. A physician can order the inserts through a pharmacy. The patient places the insert in the inferior fornix of the eye, the area between the lower lid and sclera of the eye. It slowly dissolves over 24 hours, giving constant lubrication.
Anti-inflammatory Treatments
Inflammation is now being recognized as a major underlying cause of chronic and worsening dry eye disease. Many patients who have been suffering from chronic dry eyes, particularly those with autoimmune diseases like Sjogren’s Syndrome, will do well on treatments that reduce the amount of inflammation in the tear film and ocular surface. Your physician can order these medications for you if needed.
Cyclosporine A (Restasis)
The FDA approved Restasis for dry eyes in 2002. This is an immunosuppressive and anti-inflammatory eye drop medication. Relief is not instant, and may take 6-8 weeks of sustained use for improvement in dry eye symptoms. Less than 20% of patients may experience a burning sensation with the drops, but the safety and tolerability profile is otherwise excellent.
Antibiotics
Doxycycline and minocycline are used for inflammatory ocular surface and eyelid disease. The antibiotics have a dual effect: they act as anti-inflammatories and anti-microbials. As an anti-microbial, these medications can improve meibomian gland function. They can decrease lid bacterial flora, reducing a cause of meibomian lipid breakdown. A low-dose (doxycycline 20 mg BID) regimen for 1-2 months has been shown to be effective. Side effects are usual mild but include stomach upset, yeast infections, and photosensitivity.
Steroids
Steroids act as anti-inflammatories. Because steroids are associated with complications in long-term use, they are mainly used in short pulses either at the initiation of treatment or as rescue during exacerbations. A short 4-6 week course is generally well tolerated as a “rescue treatment,” or an urgent treatment, to relieve intolerable symptoms quickly before resorting to other treatment options.
Meibomian Gland Treatments
Meibomian glands produce oils that are crucial in preventing our tears from evaporating too quickly. Treatments that target the glands can help patients with meibomian gland dysfunction or lid margin disease.
Warm compresses and lid scrubs
Warm compresses provide heat that warms the oils in the glands, unclogging the glands and improving oil flow. Warm washcloths, small rice bags heated in the microwave, or commercial hydrogel pads are all effective, and no studies have been done to compare the different methods. The heat. The compress should be placed over the eyes for 5-10 minute. Gentle circular or rolling massage of the eyelids can help express the oils from the glands.
Lid scrubs are useful particularly in cases of blepharitis, or mild inflammation of the lids, that cause them to become crusted. There are excellent over the counter commercial lid soap formulations that work well to clean the lid margins. Alternatively, baby shampoo and a washcloth gently applied to the lids can work as well.
Thermal pulsation (Lipiflow)
Lipiflow is an FDA approved in-office treatment for meibomian gland dysfunction and dry eyes. During the 12-minute procedure, a device is placed over the eye and eyelids that provides localized warmth and pressure on the lids (Figure 1).
Image 1 – Lipiflow treatment
The procedure is 100% safe and very effective at clearing out the trapped oil glands and allowing smooth flow to be re-established. After approximately one month, the consistency of the oils in the tear flow will have improved remarkably with associated improvement in dry eye symptoms. With one procedure, the effects last between 12-24 months.
Intense Pulsed Light (IPL)
Originally approved for acne and rosacea dermatologic disease, IPL uses bursts of light to minimize blood vessel size. It can be used off-label for ocular rosacea and meibomian gland dysfunction, but results have not been reported.
Summary
There are many treatment options for dry eye disease. Generally, conservative over-the-counter treatments should be tried first. Commonly, environmental changes, dietary changes, artificial tears, and warm compresses will improve the majority of dry eye symptoms to tolerable levels. However, when these options are exhausted, there are many additional options for patients. Work closely with a trusted health professional to determine the optimal treatment combination as each patient is different.
8/25/15
Marjan Farid, MD
Director of Cornea, Cataract, and Refractive Surgery
Vice-Chair of Ophthalmic Faculty
Director of the Cornea Fellowship Program
Associate Professor of Ophthalmology
Gavin Herbert Eye Institute, University of California, Irvine
As covered earlier by Dr. Wade, the symptoms of dry eye disease (DED) can be variable. Simply put, dry eyes can be separated into two categories: aqueous tear deficient (ATD) or dysfunctional tear syndrome (DTS). More commonly there is a combination of the two that I like to refer to as ocular surface disease (OSD). Lucky for you, as clinicians, we have several tools that will allow us determine what type of DED you have.
Steps In A Dry Eye Diagnosis
First is a review of your symptomatology. This is crucial to determining if you 1) have DED, and 2) what type you have. This determination can drive our treatment plan that is individual to you. In addition, we utilize various questionnaires that can help us hone in on your OSD.
Second is the ocular examination. We use a microscope (slit-lamp) to carefully examine the surface of the eye. When we look at your tear film we are looking to see the amount and health of your tears, how well they are working, and what effect they are having on the ocular surface (conjunctiva and cornea). Not only do we look at your tears, but we pay special attention to your eyelids. In your eyelids, there are oil producing glands called Meibomian Glands. These glands are responsible for creating a key component to the tear film: lipid. Human tears are very complex, but simply put, tears have 3 main components – water, mucus, and oil. I like to describe tears like salad dressing. In order to have tasty salad dressing, there needs to be a balance of oil, vinegar, and spices. Human tears are very much similar. In order for your tears to work properly, There needs to be the proper balance of the aqueous component (water), lipid component (from the Meibomian glands), and mucus component (image 1).
Image 1 – A relatively healthy meibiomian gland examination
If there is an imbalance in your tears, this will reflect in their function, and ultimately cause signs and symptoms of ocular surface disease. To highlight the appearance and function of the tears on the ocular surface, clinicians often use special stains that can aid us in determining the amount and function of your tears. Two of the most common stains are fluorescein and lissamine green. Each of these stains has particular characteristics that help determine the severity and extent of your ocular surface disease. For example, if you have significant staining near the bottom part of your cornea, your eyes maybe slightly open when you sleep, and therefore you may benefit from using an ointment at nighttime. Alternatively, if your tears appear to break up very quickly on your ocular surface, there is likely an imbalance in the tear composition that may benefit from institution of warm compresses along with tear replacement in the form of artificial tears.
Third is the use of ancillary testing to help confirm our clinical diagnosis. We are fortunate to have access to several commercially available OSD diagnostics at the Gavin Herbert Eye Institute. A brief description of if you have these diagnostics follows.
1) Schrimer Testing – This is a very simple and common method of determining whether a patient has hey aqueous tear deficiency. Essentially, the eye is numbed and a sterile piece of special paper is placed in the lower outer corner of the eye. After a specified amount of time, the amount of tears is recorded, and if under a threshold value (generally 10 millimeters at five minutes) there is a high suspicion of aqueous tear deficiency. Treatments for this subtype of OSD will be covered in the next blog.2) Tear osmolarity – The most available tear osmolarity system is from TearLab. With this test, we look at the integrity of the tears by determining the osmolarity – essentially the ultrastucture of the tears. If the tear osmolarity is high (hyperosmolar), we know that the tears are not functioning properly. With proper institution of treatment, the osmolarity can normalize indicating a healthier tear film. This test is very noninvasive, requiring only a tear sample of 50 nanoliters – less than the volume of a single tear!3) InflammaDry – Inflammation has long been accepted as a hallmark of dry eye disease/ocular surface disease. As such, many of our treatment modalities have focused on treating ocular surface inflammation (discussed in the next installment of this blog). Prior to having access to the InflammaDry test, we would have to assume that there was inflammation involved in an individual’s OSD. Now, however, we can test the ocular surface for inflammatory markers and have an answer within just a few minutes. This test not only allows us to custom tailor treatments to an individual, but also we are able to see if our treatments are working. Again, this test is minimally invasive requiring the small sample of tears for testing.4) LipiView II – This test allows us to Image of the structure and function of the meibomian glands in vivo. The images obtained allow for several things. First, we are able to determine the extent of meibomian gland dysfunction. Second we are able to determine the extent of meibomain gland drop out (image 2).Image 2 – Significant dropout of meibomian glandsAnd third we are able to educate our patients so they can see the importance of treatment of their MGD. Again, this information can help us custom tailor treatment options for the individual patient.
In conclusion, as you can see diagnosis of ocular surface disease can be quite intricate. We are fortunate to be in and age where there has been significant improvements in our tools to help us better diagnose our patients and use this information to individualize treatment options. Stay tuned for the next installment of this blog focusing on treatments for ocular surface disease.
8/20/15
Sumit “Sam“ Garg, MD
Medical Director and Vice Chair of Clinical Ophthalmology
Assistant Professor of Ophthalmology
Gavin Herbert Eye Institute – UC Irvine
If you could be a fly on the exam room wall of your local ophthalmologist, you would hear patient after patient report symptoms of dry eye disease.
Some patients come in already knowing they have dry eyes. However, the variability of symptoms that can occur from dry eye disease is so wide many patients don’t even use the word “dry.” We will cover some of these symptoms in this article.
Redness often associated with dry eye
Underlying Factors
Dry eye disease has many underlying factors including an inadequate production of tears, rapid evaporation of tears, poor eyelid function and an imbalance in the tear composition of water, oil, and mucus. Dry eye disease can be associated with systemic conditions such as Sjogrens disease, Sarcoid disease and sleep apnea among many others. It is more common in females especially after hormonal changes such as menopause.
Exacerbating Influences
Many medications can exacerbate dry eye disease. Over the counter antihistamines are one example.
Environmental factors may also worsen dry eye symptoms. These include dry climates, windy weather conditions, smoky environments and the dry air found in airplanes.
Modern life includes hours and hours of focusing our eyes on everything from cell phones to computer screens to television. Prolonged focusing reduces the blink rate resulting in more tear evaporation and worsening of dry eye symptoms. Increased evaporation can also occur with exposure to heating, air conditioning, fans and rolling down the car windows while driving.
Symptoms Fluctuate
It is very common for dry eye symptoms (especially blurred vision) to wax and wane throughout the day. Symptoms can even change from blink-to-blink. Dry eye disease which is predominately due to insufficient tears tends to worsen throughout the day with symptoms worse at night. Dry eye disease that is more associated with blepharitis can be worse in the morning. Blepharitis is associated with burning and itching of the eyes.
Visual Symptoms
The front surface of the eye is the most powerful focusing surface of the eye. Thus, a dry ocular surface will produce visual symptoms. These symptoms can include:
Blurred vision: A decrease or fluctuation in visual acuity. This is manifested in the inability to see fine detail. Objects at both near and far may appear out of focus.
Sensitivity to light: Sensitivity to light is termed photophobia. It occurs because a dry ocular surface has more irregularities than a health surface. These irregularities scatter light entering the eye. This scattered light can cause significant discomfort. The inability to tolerate light may lead to squinting and headaches.
Difficulty with nighttime driving: During low light conditions, such as at night, the pupil enlarges and allows more light into the eye. When the ocular surface is dry, the incoming light becomes unfocused and scattered. Many of these abnormalities are filtered out by the small size of the pupil during the day. However, at night, the larger pupil size allows more light abnormalities to pass through to the retina. This results in nighttime glare and halos. Glare is a decreased tolerance of bright lights. Halos present as circles or auras around a bright source of light. Glare and halos from the headlights of oncoming traffic are especially troublesome.
Physical Symptoms
The front surface of the eye is richly supplied with nerve endings. As such, a dry ocular surface can result in significant symptoms of discomfort. In addition to feeling dry, these symptoms include:
Foreign body sensation: Patients may feel as if there is something present in the eye.
Redness of the eye: Enlarged blood vessels on the ocular surface cause the eye to look red.
Ocular and periocular pain: Pain from dry eye can be mild or severe. Pain from dry eye can be felt on the ocular surface. Pain can also be felt in structures around the eye such as the eyelids or scalp.
Periocular irritation: Stinging, burning, or itching sensations of the ocular surface and eyelids.
Watery eyes can be a symptom of dry eye
Watery eyes: Patients typically raise an eyebrow or two when I explain how the tearing they are experiencing is from dryness. “How can my eyes be dry if they are watering all of the time?” Although this may seem counter-intuitive, when the ocular surface is very dry it will overproduce the watery component of the tears as a protective mechanism.
Eye fatigue: A tired sensation of the eyes and heaviness of the eyelids.
Decreased tolerance of sustained visual focusing: As noted earlier, any activity that requires prolonged visual attention will decrease the blink rate and increase tear evaporation.
Discomfort while wearing contact lenses: Individuals may experience pain and irritation in the eyes while inserting or wearing contact lenses.
Inability to cry: Tears associated with emotional discomfort or watching a sad movie may be decreased in some types of dry eye disease.
Stringy discharge from the eye: A dry ocular surface can result in the overproduction of a sticky, mucus discharge.
Conclusion
There are many symptoms of dry eye disease. Some symptoms affect vision and others affect ocular comfort. If symptoms persist, an evaluation by your eye care provider can help clarify the cause and offer information on treatment options.
It is important to remember the symptoms of dry eye disease can overlap with the symptoms of other ocular conditions. One example is cataracts which, like dry eye disease, can also cause blurred vision and nighttime glare. The next post in this series will review how dry eye disease (and its sub-types) are diagnosed.
As a final note, while the name “dry eye disease” may sound innocuous, the symptoms of dry eye disease can be very severe in many patients. If you suffer from dry eye disease, you are not alone. Today there are many treatment options which can be very helpful. Significant research is underway to continue improving our ability to treat dry eye disease.



 Susan DeRemer, CFRE
Susan DeRemer, CFRE