Lately we have heard quite a bit about carrots and the positive effects they can have on your vision, such as slowing the progression of age-related macular degeneration (AMD). This is because carrots contain pigments called carotenoids. These pigments also give vegetables their colors, in this case orange. But carrots weren’t always orange.
The beginnings of carrots can be tracked back to the dry, hot lands of Iran and Afghanistan in 3000 BC, when the root vegetables were black, white, red and purple. They were bitter and used as a healing remedy for many illnesses, as well as an aphrodisiac.
The vegetable grew in popularity because it was still edible even after months of being stored in a variety of conditions. Carrot seeds were soon picked and sold to neighboring Middle Eastern, African and Asian populations. This is when the crossbreeding started and new types of carrots were created.
Across centuries and continents, the carrot evolved, improving the composition, look, flavor and size. After years of selective breeding, in the 17th century a Dutch yellow carrot was engineered to get rid of the bitterness, increase sweetness and minimalize the wooden core. This appears to be the origin of the orange carrot we enjoy today.
Americans didn’t fully use carrots until after World War I when soldiers returning home told about French and other European cuisine which included the carrot. However, it didn’t really become popular until World War II, when England actively encouraged home growing of carrots while the US was engaged in cultivating “Victory Gardens.”
Today the carrot is found around the world in temperate regions. They have a high nutrition value, presence of ?-carotene, dietary fiber, antioxidants, minerals and ability to be prepared in a wide variety of recipes. They have become a staple in many countries.
Currently, the largest producer and exporter of carrots in the world is China. In 2010, 33.5 million tons of carrots and turnips were produced worldwide, with 15.8 million tons from China, 1.3 million tons each from the US and Russia, 1 million tons from Uzbekistan and less than a million from Poland, the United Kingdom and Ukraine.
Because of the popularity and health benefits of carrots, they are now enjoyed in a variety of ways – beyond the simple salad. Here are some recipes you might find interesting to try:
Roasted Carrot, Squash and Sweet Potato Soup – This is a more traditional carrot recipe, it is not that hard to find a carrot soup, but this one also has squash and sweet potatoes which are also eye healthy!
Carrot Farfalle Pasta with Lemon and Herbs – Not only are carrots good for flavor, but they add a nice color to this pasta that could be the base for any number of pasta dishes.
People afflicted with keratoconus (KC) are often obligated to wear contact lenses in order to obtain functional vision. Unfortunately, wearing contact lenses can have detrimental effects on the ocular surface and tear film layers over the course of decades, ultimately reducing lens tolerance. Therefore, any intervention prolonging the comfortable wear time of contact lenses should be aggressively pursued. The tear film covers the surface of the eye, provides lubrication and is the primary defense against foreign bodies and infection. Without a robust and healthy tear film, safe and comfortable contact lens wear is not possible. This article will describe the structure of the tear film and review simple remedies that can keep it healthy throughout life.
Tear Film Layers
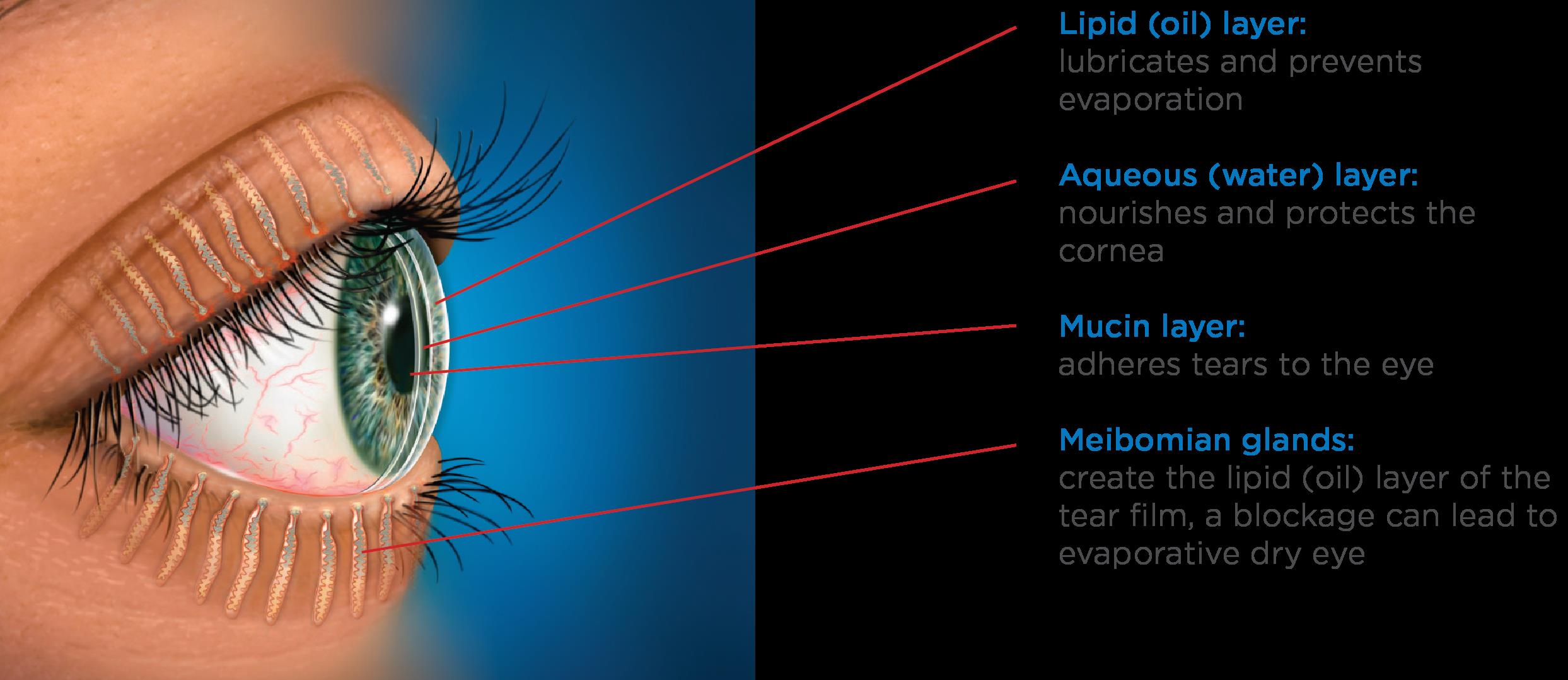
The tear film is a complex, triple layered structure comprised of mucus, water and oil. The surface of the cornea and conjunctiva contain cells specialized to secrete a sticky mucoid substance. These so called goblet cells produce the mucin layer of the tears, which creates a “Velcro” type interface and allows the overlying watery component to stick to the ocular surface without washing away.
The bulk of the tear film is comprised of the watery, or “aqueous” layer which is secreted primarily by the lacrimal gland. This specialized structure is located near the eyebrow. This gland continuously releases small amounts of watery fluid that also contains enzymes and antibodies to help fight infection and wash away contaminants.
The lipid layer is the final, outermost layer of the tears. If the tear film is the first line of defense for the ocular surface, then the lipid layer is the first line of defense for the entire tear film and the ocular surface combined. Because of that role, it is extremely important and helps stabilize the tear film by preventing evaporation. This thin, lipid based layer is released by the meibomian glands, which are modified sebaceous glands that reside in the upper and lower lids. In each lid there are 20-30 glands. These glands open up onto the lid margin and through the action of a complete blink, release the lipid secretion to ocular surface which gets spread with the upward motion of the upper eyelid.
Each one of these layers contributes to the structure of the tear film, and a problem with any one of these structures (goblet cells, lacrimal gland or meibomian glands) will negatively impact the corresponding tear layer. Image 1 -Layers of the tear film across the ocular surface & Meibomian glands of the eyelids. (Picture courtesy of TearScience™)
Tear Film Issues
Because the tear film is so thin, each individual component is necessary to maintain the integrity of the tears as a whole. When any layer of the tear film is deficient, the tear film becomes unstable and the ocular surface becomes irritated and can progress to developing classic symptoms of dry eye. This includes burning, stinging, redness, tearing, fatigue and contact lens intolerance.
Deficiencies in the mucin layer are uncommon, and are typically the result of chemical or thermal insult, or scarring. An aqueous deficiency, primarily from a lacrimal gland related etiology, is also relatively uncommon, and can arise from autoimmune and inflammatory causes such as Sjögren’s Syndrome. The most common reason for a poor tear film is linked with excessive evaporation of our tears due to a lack of sufficient lipid secretions from non-functioning or obstructed meibomian glands. It is understood that many factors contribute to why these glands stop performing optimally.
One factor has been linked to our habitual working environments. The compressive force exerted by the muscles of our eyelids that control blinking are essential for lipid secretion. However, the use of computers or wearing contact lenses has been shown to negatively impact our blinking habits, both by reducing the number of blinks and making blinks less complete. With an incomplete blink, the upper and lower lids do not make contact. The negative consequences of this are 1) the meibomian glands do not release their lipid contents, 2) the lower part of the eye is chronically exposed to the air, increasing evaporative stress and 3) dead skin cells accumulate on the lid margin which can clog the meibomian gland openings.
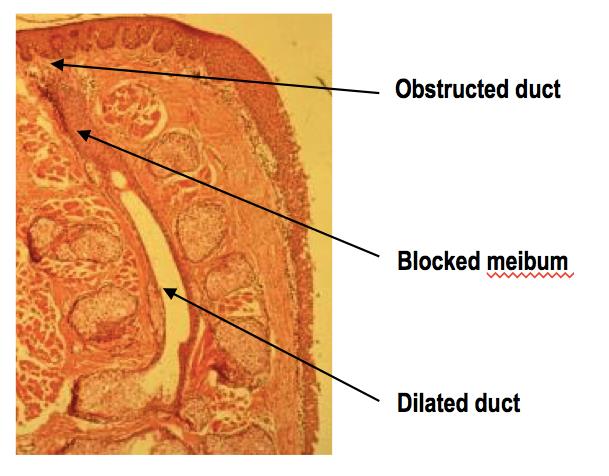
When increased evaporation of the tear film occurs chronically, the integrity of the entire ocular system becomes compromised over time and problems to the health of the eye become permanent attributes. This condition is known as Meibomian Gland Dysfunction or MGD and is linked with 86% of all dry eye sufferers. Image 2 – Histology slide of a Meibomian gland with a terminal duct blockage
Contact lenses have been shown in multiple studies to have a negative impact on the integrity of the tear film. To begin with, placement of a lens onto the eye divides the tears into two sections, referred to as the “post” (behind) and “pre” (in front) lens tear films.
The characteristics of the post lens tear film can differ depending on the type of lens that is worn. For example, soft lenses and scleral lenses have very little turnover of this post-lens tear film. This can cause issues related to the build up of toxic waste and bacterial elements that ultimately aggravate the corneal surface. Conversely, rigid gas permeable lenses are designed to have substantial tear turnover behind the contact lens with every blink.
The pre-lens tear film is also greatly affected by the type of lens material, as well as the interaction between the lid and the contact lens surfaces. Eye doctors know that without a healthy tear film, chances for contact lens intolerance increases. The rate of contact lens intolerance substantially increases as patients enter their fourth decade of life, primarily because of MGD caused by years of poor blinking habits.
Tear Film Care
Fortunately, simple interventions can prevent and/or limit the severity of MGD altogether or help to manage it once it occurs. Just like brushing and flossing one’s teeth can prevent gum disease, attention to complete blinking and lid margin hygiene can improve the tear film and prevent contact lens intolerance problems.
Because partial blinking is strongly linked with developing MGD, it is vitally important that the two lids touch when blinking. It is best to practice this several times throughout the day as well as when you are reading or using the computer.
Akin to flossing the teeth, it is also important to clean the lid margins with a Q-tip soaked in saline solution or a bit of mineral oil by gently brushing the Q-tip across the lid margin 10-20 times each night. It is easiest to get the lower lid.
Finally, performing warm compresses daily can provide heat to the Meibomian glands to soften the hardened oil that can plug the meibomian gland ducts. Warm compresses need to be done continuously for at least 10 minutes with consistent heat in order to attain a temperature that is sufficient to melt the oil that clogs the glands. We recommend folding 5-6 small towels or facecloths into a rectangular shape and wrapped together into a circular bundle, similar to the appearance of a cinnamon roll. The towels should be damp and moist, placed in a microwaveable safe dish with a lid and heated for approximately 1 minute and 50 seconds. After removal, wait a minute or two and then proceed to use the outermost cloth and cover the rest. Replace the first cloth after two minutes and grab the next outer most towel from the bundle, continuing this until all towels are used. In this way, the temperature can be adequately maintained for the full 10 minutes. The high temperatures applied to the lid are transferred to the cornea and very often cause temporary deformation, a phenomenon characterized by transient visual blur immediately following compress application. Therefore, it is vitally important, especially for patients with keratoconus, that pressure never be exerted onto the globe of the eye with a compress or massage administered to the lids of closed eyes after a compress.
It is becoming apparent that MGD is developing in patients at earlier ages. Because of this, the condition has likely been present for decades by the time the patient becomes symptomatic. It may take significant time and effort to rehabilitate not only the glands themselves, but also to reduce the resulting inflammation of the ocular surface.
Meibography is the technique used to image Meibomian glands. In chronic cases of MGD, we see abnormal changes to gland structure, in the form of atrophy or loss of gland tissue and/or dilation of glands where obstructed material causes glands to become widened. In severe cases, the prognosis for recovery is guarded.
The visual clarity that contact lenses provide for patients with keratoconus is incredibly important. But the ability to comfortably wear contact lenses is reliant on our body’s ability to provide a sufficiently thick protective tear film. Taking a small amount of time daily to attend to the lipid producing Meibomian glands by proper blinking habits, exfoliation of the lid margin with a Q-tip and warm compresses will help to extend the number of hours, and ultimately the number of years, that contact lenses can be safely and comfortably worn.
10/20/15
Amy Nau, OD
Korb and Associates, Boston, MA
Contact lens fitting for keratoconus, other ocular surface disorders and dry eye
The following is a survey done by Essilor (a French company that produces ophthalmic lenses along with ophthalmic optical equipment) and a large marketing research firm in the UK, YouGov. While the focus in on people living in the UK, the results would probably be similar to the US population. Even with increased access to the Internet, many people are still not aware of the risks associated with eye disease and what they can do to help retain their vision. Increased awareness of informational resources are important for saving vision.
There are a number of websites with easy to understand information about taking care of your vision that I have listed under Resources to Help Save Vision at the bottom of this article. And while there are eye diseases that are hereditary, you can slow the onset and progression by making good lifestyle choices about smoking, diet and exercise. Your eye care specialist is also an excellent source of information about what you can to do reduce your risk of vision loss, at any age.
Increased Awareness for Saving Vision
A YouGov poll conducted with Essilor reveals that most Britons are unaware of damage to their eyes by surrounding objects, activities, and devices. This widespread lack of awareness means fewer people seeking methods of prevention and avoidance, and for those that are aware of risks, most are not informed of existing preventative measures.
The poll has shown* that many British people remain uninformed about the various ways in which eyes are damaged by common daily factors, despite evidence that eye health is affected by blue light, UV rays (reflected from common surfaces), diet, obesity, and smoking.
Of the 2,096 people polled, the percentage of respondents aware of the link between known factors affecting and eye health were:
Poor diet – 59%
Obesity – 35%
Smoking tobacco – 36%
UV light, not just direct from the sun but reflected off shiny surfaces – 54%
Blue light from low energy lightbulbs and electronic screens – 29%
More than one in ten people were completely unaware that any of these factors could affect your eyesight at all.
72% of respondents own or wear prescription glasses but only 28% knew that there were lenses available (for both prescription and non-prescription glasses) to protect against some of these factors; specifically, blue light from electronic devices and low energy light bulbs, and UV light from direct sunlight and reflective surfaces.
76% admitted they haven’t heard of E-SPF ratings – the grade given to lenses to show the level of protection they offer against UV.
Just 13% have lenses with protection from direct and reflected UV light, and only 2% have protection from blue light (from screens, devices, and low energy bulbs).
Poll results showed that younger people were most aware of the dangers of UV and blue light, yet least aware of how smoking tobacco and obesity can affect your eye health. Within economic sectors, middle to high income people are more aware of the effects of smoking & obesity on eyesight than those with low income –
39% of people with middle to high income compared to 33% of people with low income are aware of the impact of smoking tobacco.
38% of people with middle to high income compared to 31% of people with low income are aware of the impact of obesity.
Awareness of the impacts of smoking and obesity on eye health is significantly higher in Scotland (47% & 49% respectively) than anywhere else in the UK (35% & 33% in England and 40% & 38% in Wales).
Essilor’s Professional Relations Manager, Andy Hepworth, has commented: “The lack of awareness about these common risks to people’s eyes is concerning. Not only would many more glasses wearers be better protected, but also many people who do not wear glasses would likely take precautions too, if made aware of the dangers and the existence of non-prescription protective lenses.”
To see the full results of the poll, please visit the Essilor website.
For more information on the protection offered from blue light and UV through specialist lens coatings, for both prescriptions and non-prescription glasses, please see here for UV & Blue Light Protection options.
*All figures, unless otherwise stated, are from YouGov Plc. Total sample size was 2,096 adults. Fieldwork was undertaken between 21st and 24th August 2015. The survey was carried out online. The figures have been weighted and are representative of all GB adults (aged 18+).
Food for Thought – Business Opportunity for Blind Adults
For those not in the know, the acronym sounds like a popular sandwich. However, for Louisville, KY resident, George Bouquet, The Hadley School for the Blind’s and the National Association of Blind Merchants’ joint“BEPLT” program (Business Enterprise Program Licensee Training) is more like a dream come true.
George Bouquet
Hadley is the largest provider of distance education for people who are blind and visually impaired worldwide and the BEPLT program is part of the school’s Forsythe Center for Employment (FCE) and Entrepreneurship. Under the Randolph-Sheppard Act, legally blind adults are given first right of refusal on operating state and federal government vending facilities including cafeterias, snack bars, convenience stores, micro markets, and vending machines and rest stop vending areas nationwide. In February 2014, Hadley’s FCE partnered with the National Association of Blind Merchants (NABM) and the National Federation of the Blind Entrepreneurs’ Initiative (NFBEI) to bring the academic portion of training to would-be blind vendors. Individual state Business Enterprise Programs provide the hands-on component of the blind vendor training. Bouquet is Hadley’s first graduate from the school’s new BEPLT program.
Born with both Pierre Robin Syndrome, which often results in a smaller-than-normal lower jaw, a cleft palate, a tongue that falls back in the throat, and difficulty breathing, as well as Stickler Syndrome, which causes hearing loss, eye abnormalities and joint problems, Bouquet has struggled with health issues throughout his 54 years. Although he was born without eye lenses, he was not born blind. Rather, his vision worsened over time. Bouquet worked in several food service positions since high school and had wanted to become a Randolph-Sheppard vendor even before he would have qualified as legally blind!
There are only so many blind vendor licensee training slots available and many more people compete for them than such programs can accommodate. The first time Bouquet applied to receive the training was in February 2014. Unfortunately, he was not accepted into a program. However, he was fortunate to gain some blind vendor experience by working under friends who already held the license. In early 2015, Bouquet’s counselor told him of another opportunity to apply for vendor training. This time he was accepted and Bouquet began Hadley’s BEPLT program in April 2015. Bouquet was so motivated to graduate from the program that he completed approximately two modules (one-lesson online courses) per week. Hadley’s BEPLT students complete a 10-module program and then take their state’s physical training component. After passing both elements, graduates are eligible to bid for the opportunity to become a blind vendor in their community.
“The [Hadley BEPLT] program offers a lot of useful information. It will really help anyone wanting to undertake vending,” he said. Bouquet then acknowledged that the material about food borne illnesses helped him to realize the tremendous responsibility he would be accepting by running a government food service area. “As a manager, you need to decide what you are willing to delegate to other people,” he added.
For Bouquet, becoming a blind vendor allows him to hire and train his 25 year-old unemployed son, who inherited most of his visual and hearing problems. This training is Bouquet’s first step toward creating a legacy of financial independence.
This article is reprinted with the permission of Dr. Kenneth W. Wright, Medical Director of the Wright Foundation for Pediatric Ophthalmology & Strabismus. Check out his website for information on over 20 pediatric eye disease and conditions.
Normal Binocular Vision
Normally, both eyes are aligned on the same visual target and the images from each eye are merged in the brain to form a single three-dimensional image, or binocular vision. The brain’s process of merging or “fusing” images from each eye into one image is called binocular fusion. The perception of three-dimensional depth is called stereoscopic vision. Stereoscopic vision is the highest level of binocular vision and requires intricate processing of information from both eyes. Binocular vision develops during early infancy, and proper alignment during this time is necessary for normal binocular development to occur.
Accommodative Esotropia
Esotropia means one eye is turned in towards the nose, or crossed eyes. Patients with esotropia have one eye aligned on the visual target, but the other eye is turned in towards the nose. When the eyes are crossed only one eye is aligned with the target and the child is forced to use only one eye for vision. Accommodative esotropia is a type of esotropia caused by significant farsightedness (hypermetropia). Most think that farsighted people can see well only in the distance. In children, this is not true. Children have the ability to focus great amounts, so most children can see well for distance and near even without glasses. Focusing (medically termed accommodation) is the process of increasing the lens power of the eye to see clearly. Linked to focusing is the natural reflex of convergence (eyes move in). As one focuses on an approaching near object, the eyes move in to stay on target. This process of focusing and convergence used for near vision is termed the near reflex. Accommodative esotropia occurs because the farsighted child has to over focus to see clearly. When eyes over focus, the natural reflex is for the eyes to cross. You can experience this by trying to see the tip of your nose. When you look at the tip of your nose you have to over focus and consequently your eyes cross. Since more focusing is needed to see near objects, the crossing tends to be greater when looking at close objects. Right eye turns in because patient is farsighted and not wearing glasses.Eyes are in excellent alignment after prescribing glasses.
The onset of accommodative esotropia is most commonly seen between the ages of 2 and 4; however, even infants can have crossed eyes. This situation is usually first noticed when the child is tired, sick, or looking at an object very near to their face. Some children cross when they are tired and this is because they cannot sustain the effort to keep the eyes straight. The crossing is usually intermittent at first, but can quickly become constant. There may be a parent or a close relative with the same problem; however, in many cases there is no family history of crossed eyes.
During the examination, three important determinations are necessary. The first determination is to make sure the vision is normal in each eye. This is done by assessing the visual behavior of the preverbal child, or simply having the verbal child read the eye chart. Secondly, the amount of crossing is evaluated. This is measured using prisms while the child is viewing an object. Thirdly, the need for glasses is measured, and this requires drops to dilate the pupil and relax the child’s focusing. These drops take approximately 20 to 30 minutes to work and will blur vision for 1 to 3 hours, but the pupil may stay large for much longer. After the eyes have been dilated, the eyeglass prescription is calculated using a special light (retinoscope) along with lenses. Determining the proper lens power in young children is difficult and may require repeat exams and changes in the eyeglass lenses.
Effects of Esotropia on Visual Development
Esotropia occurring in young children and infants results in the immature brain turning off the information from the deviated eye. This mechanism of turning off visual areas of the brain connected to the deviated eye is called “suppression.” Thus, patients with esotropia use one eye at a time (monocular vision) and do not have binocular fusion or stereoscopic vision. Suppression disrupts normal binocular visual development and if not treated early, causes permanent loss of binocular vision and stereoscopic vision. Early treatment of esotropia is critical to stimulate binocular development.
How Do Patients with Esotropia See?
If the esotropia is acquired in late childhood (after 7 to 9 years of age) or in adulthood, it will cause double vision. Esotropia occurring in infants and young children, however, does not cause double vision, as the young, immature brain has the ability to suppress the information from the deviated eye. The child uses one eye at a time to see and avoids double vision. The fact that the eyes are crossed disrupts normal binocular visual development and often causes permanent loss of binocular vision and stereoscopic vision. Early treatment of esotropia is critical in order to stimulate binocular development.
Treatment of Accommodative Esotropia
Glasses
The goal of treatment is to align the eyes, stimulating them to work together to establish binocular vision and stereoscopic vision. Children and infants who are significantly farsighted are best treated with glasses. If the glasses align the eyes, then surgery is not necessary, and the treatment is to continue with the glasses. The full, hypermetropic (farsighted) prescription is usually given via eyeglasses, and most parents are surprised at how well these children adjust to the glasses. When properly worn, most children adapt to the glasses like “fish to water.” The glasses not only straighten the eyes, but also relax the child’s vision, as they no longer have to over focus. In patients with accommodative esotropia, glasses must be worn full-time. Older children over 4 to 5 years may have blurred distance vision when they first put on their glasses. This is because they had a strong habit of over-focusing and continue to do so even when wearing the glasses. Over several days, most children will relax their over-focusing and enjoy the comfort the glasses afford. In those children who do not adapt to the glasses, drops can be used to relax focusing, or a reduced prescription power can be given. In most cases, however, the best treatment is to give the full power. The eyes usually straighten within a few days to a few weeks after wearing the glasses. If the eyes are still crossing with the glasses and the child is not using the eyes together after several weeks, then eye muscle surgery is usually required. Occasionally, an initial response to glasses is that the eyes “break down” and cross for distance and near. In this situation, surgery in addition to the glasses may be required.
Bifocal Glasses
In certain children, glasses will align the eyes for distance viewing, but the eyes will still cross for near work. These patients can be helped with bifocal glasses. A bifocal is a small powerful lens placed in the lower part of the eyeglass lens. This more powerful lens will further relax near focusing to straighten the eyes for near work. Chin-up posturing for near work indicates that the child is using the bifocals correctly and is viewing through the bifocal lens for near work.
Amblyopia
Some children with crossed eyes have a strong fixation preference for one eye (dominant eye) and constantly have one eye turned in. Constant use of only one eye can lead to vision loss of the deviated, or non-dominant, eye. Poor vision occurs as visual areas in the brain connect with the dominant eye and are then subsequently suppressed. If left untreated, the deviated eye will progressively lose vision over time. This poor vision caused by brain suppression is called amblyopia. Amblyopia occurs only in young children when the visual areas are immature and still developing. Children who have a difference in the strength of the glasses in one eye as compared to the other have an increased risk of developing amblyopia in the more farsighted eye. Approximately 20 to 40% of patients with esotropia will also have amblyopia of the non-preferred eye.
Patching
If amblyopia is present, patching of the good eye is indicated to promote visual stimulation of the amblyopic eye and improve vision. Patching does not straighten the eyes and is not indicated if vision is equal. Another way to promote stimulation of the amblyopic eye is to blur the vision of the “good eye.” This can be done by placing a blurring lens over the good eye, or by administering drops to blur the good eye. In most cases, patching the good eye with an adhesive patch is the most practical treatment. Patching is continued until vision improves in the weaker eye, usually taking a few weeks to several months. In the vast majority of patients, vision can be improved if the parents and child are compliant with the treatment.
10/8/15
Kenneth W. Wright, MD
Medical Director, Wright Foundation for Pediatric Ophthalmology & Strabismus
Clinical Professor of Ophthalmology, USC Keck School of Medicine
On Tuesday, September 29, 2015, the National Eye Institute(NEI) hosted a Twitter chat on vision loss and depression. Here are some highlights of that discussion, along with some great resources to learn more about dealing with vision loss and depression.
Many studies show that people with vision loss or low vision are at risk for depression, although not everyone with vision loss gets depressed.
A person with low vision is defined as someone who finds it difficult to do daily tasks even with regular glasses, contacts, medications or surgery.
The number of Americans with low vision will increase over 70% by 2030. Broken down by ethnicity, African Americans with low vision will increase 93% and Hispanics with low vision will increase 190% during the same period. This is due to the rapidly aging Boomer population. 88% of Americans with low vision are age 65 and older.
Symptoms of depression include persistent feelings of sadness, anxiety, irritability and fatigue. It is a common and serious illness that interferes with daily life. Each year, about 6.7% of American adults experience major depressive disorder. Women and men experience depression differently, with women 70% more likely to experience depression than men.
People 65 and older are at particular risk for developing serious depression related to vision loss and yet it is often underdiagnosed and undertreated. Older adults may have other, less obvious symptoms of depression or they may not be willing to talk about their feelings. Many overlooked because sadness is not their main symptom. It is important to remember that while depression is a common problem among older adults, it is not a normal part of aging.
An estimated 29-58% of those who suffer significant vision loss have major depressive disorder one year later. People with vision loss are 2x more likely to be depressed than someone without vision loss. Depression can be very disabling and may reduce the effectiveness of low vision rehabilitation interventions.
A recent study confirmed age-related macular degeneration (AMD) is a big contributor to depression risk, as it accounts for about 45% of low vision cases.
Older adults w/ vision loss are also 3X more likely to report difficulty in 1) walking, 2) managing medications, and 3) preparing meals. In fact about 39% of people with severe vision loss experience activities of daily living ADL limitations, compared to 7% of those with better vision. ADLs include eating, bathing, dressing, toileting, walking and continence.
A link between depression and vision loss was also found in people as young as 20 according to a recent study. It looked at over 10,000 adults in the US and found they were approximately 2x more likely to be depressed.
A decline in vision can also be associated with lower emotional, physical, and social functioning. To help those with low vision avoid depression it is important that they remain active and engaged in the world around them. And while people may become depressed because of vision loss, other causes of depression may also be present.
An integrated approach to depression management in older adults with impaired vision may be the best course of action. Behavioral activation helps people recognize that loss of the activities they enjoyed that have led to depression and encourages them to find ways to re-engage with these activities. After 4 months, behavioral activation reduced the risk of depression by 50% compared to the control group. Behavioral activation can be used alone, or as part of psychotherapy called cognitive-behavioral therapy (CBT).
Cognitive behavioral therapy (CBT) helps people with depression restructure negative thought patterns and to correct distorted thinking that is often part of depression. But it is important to remember that the best approach to treating depression is to personalize it for each individual.
Often, the combination of pharmacotherapy and psychotherapy is a very effective option for depression treatment. Other time-limited psychotherapies, including interpersonal therapy (IPT) are effective in treating depression in people of all ages.
Collaboration between eye care and mental health professionals can help people with vision loss improve their quality of life.
Glaucoma in children includes a variety of disorders in which drainage system of the eye does not function adequately, leading to abnormally high pressure inside of the eye (the intraocular pressure, or IOP), and resulting in damage to many different structures of the child’s eye. If not treated promptly and successfully, pediatric glaucoma can lead to severe vision loss or even blindness in one or both eyes. In primary childhood glaucoma, the drainage system usually has not formed properly (often resulting from a genetic abnormality) while in secondary childhood glaucoma, the abnormal fluid outflow problem results from other problems with the eye(s), sometimes accompanied by other medical problems outside the eyes.
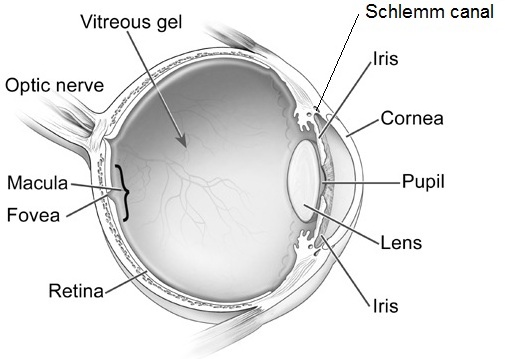
Primary congenital glaucoma is the most common of the primary childhood glaucoma types, although it is still rather rare. Let’s take a moment now to review the parts of the eye, and eye’s drainage system, sometimes also called the “aqueous outflow pathway”, since it drains the fluid within the eye (the aqueous humor), which is separate from the tears that flow on the outside of the eye’s surface and then into the nose or down a child’s cheeks.
The aqueous outflow pathway of the eye (comprising both the trabecular meshwork and Schlemm canal), situated at the junction (or “angle”) between the iris (the colored portion of the eye) and the sclera (the white part of the eye), has not formed correctly (Figure 1).
Figure1. Schematic eye shows different structures of the ocular globe. Note that the Schlemm canal is part of the drainage system of the eye . Modified from National Eye Institute.
The aqueous humor therefore builds up within the front portion of the eye, causing abnormal elevation of the IOP.
In contrast to the eyes of adults and older children, the entire eye in infants and young children is distensible and the high IOP in primary congenital glaucoma often causes stretching and damage to several parts of the eye; this most often results in enlargement, clouding and scaring of the cornea (the front window of the eye) as well as severe nearsightedness, damage to the optic nerve, and resulting poor vision.
Primary congenital glaucoma (also called PCG) is almost always genetic, although usually there is no one else in the family with the condition. It is not related to anything that the parents did (or did not do) during the pregnancy or afterwards, and does not have any relationship to the baby’s sex or racial background. It occurs in about 1 every 10,000 to 20,000 births in western countries, but may be more common in certain populations of the world. Most babies with this disease are otherwise normal.
How is primary congenital glaucoma diagnosed?
Most cases present within six months of birth, with nearly 80% presenting before one year of age. In 70- 80 % of cases both eyes are affected. Most cases present for medical attention due to the size or cloudy appearance of the cornea in one or both eyes (Figure 2).
Fig 2. Left eye of child with congenital glaucoma. The eye is enlarged and the front part of the eye is cloudy (corneal edema).
In cases where only one eye is affected, a difference in size can be seen between the two eyes and this sometimes brings the baby to the ophthalmologist (Figure 3).
Fig 3. Different size of eyes in a child with congenital glaucoma. Note the increased size of the right eye. The brown area (iris) and the transparent part in front of the color part (cornea) are significantly larger in the right eye.
The diagnosis of PCG is based on clinical findings and there are three classic signs that the child can present with:
abnormal sensitivity or intolerance to light (photophobia)
excessive blinking or squinting of the eyelids (blepharospasm)
excessive tearing (epiphora)
The exam in clinic can be challenging for infants and young children and most require an exam under anesthesia, to allow detailed examination of the eye(s) that would not be possible in the clinic. Often the ophthalmologist will be able to follow the examination under anesthesia with the most appropriate surgery for the glaucoma, if surgery is indeed required.
How is primary congenital glaucoma treated?
PCG is almost always treated with surgery, although medications are often needed to help in addition to the surgery. Medications are very useful before initial surgery to help reduce the IOP and decrease the clouding of the cornea. In addition, medications may be recommended to keep the IOP to a safe level after surgery has been performed. If the IOP is not controlled successfully, or if damage has been substantial prior to diagnosis and treatment, PCG causes severe vision loss and can even cause blindness. Sometimes the damage from PCG is uneven between a child’s two eyes, leading to amblyopia (“lazy eye”) in the more severely affected size.
The initial surgical procedure of choice is usually aimed at opening the trabecular meshwork and Schlemm canal (the aqueous outflow pathway) of the affected eye(s). This so-called “angle surgery” can be performed either from inside of the eye (goniotomy) or externally (trabeculotomy), and may need to be repeated more than once in some cases.
If angle surgery fails, other procedures are available to allow the aqueous humor fluid to exit the eye (glaucoma drainage device or filtration surgery), or even to decrease the amount of fluid the eye makes (cycloablation procedures). For these more difficult procedures, the child is usually referred to an ophthalmic surgeon with expertise in treating childhood glaucoma.
What is the prognosis for children with primary congenital glaucoma?
While vision loss can be severe, prompt diagnosis and effective treatment and follow-up for children with PCG usually allows affected children to have best-corrected vision of at least 20/50 vision in their better-seeing eye. Children with PCG require continued careful follow-up and treatment their lifetime, and may require more than one surgery, eye drops, and spectacles.
Successful care for children with PCG takes a dedicated team including the family, ophthalmologist, teacher and community support, and the child him/herself.
10/1/15
Elena Bitrian, MD
Assistant Professor of Ophthalmology, Division of Glaucoma Mayo Clinic
Sharon F Freedman, MD
Professor of Ophthalmology and Pediatrics
Chief of Pediatric Ophthalmology
Duke Eye Center, Duke University
A sure sign that fall is here is that Starbucks is offering their Pumpkin-Spiced Lattes. Since pumpkins begin to ripen in September, this makes sense. But there are so many other ways to enjoy pumpkins, which can be good for your vision.
They contain an abundance of antioxidants, vitamins, fiber and phytonutrients that are good for your skin, eyes and heart, and they may also decrease your risk of cancer.
When shopping for your pumpkin you need to look for the sugar or cheese pumpkins varieties that are good for cooking and baking, because of their dense, sweet flesh. A traditional field pumpkin that you use for decoration and carving jack-o’-lanterns has watery, stringy flesh and is not recommended for eating.
You can keep an un-cut pumpkin at room temperature for up to a month. Stored in a cool cellar or refrigerator, they can last up to three months. However, once you cut the pumpkin, pieces should be wrapped tightly and refrigerated and used within five days.
Pumpkin Season Recipes
Here are a variety of tasty recipes that will let you enjoy pumpkins beyond the traditional soup and pie (but we have included those two as well).
As the days get shorter and the temperatures cool off, these recipes will hopefully get you geared up for autumn, and the holidays that are around the corner. Let us know which recipes are your favorites in the comments below.
Just like any other organ in the body, the retina needs a healthy blood supply to function properly. When a blood vessel in the retina becomes blocked, sudden loss of vision can occur. Such blockages, known as retinal vascular occlusions, often occur in older adults. Because there are effective treatments available, seeing a specialist promptly can prevent further problems or even restore vision.
Retinal arterial occlusions
Arteries are the vessels that bring fresh blood containing oxygen and nutrients to different parts of the body. The artery that supplies the retina is known as the central retinal artery. After it enters the eye, the central retinal artery splits up into branch retinal arteries that serve different areas of the retina.
Symptoms
The symptoms of a central retinal artery occlusion include a sudden, painless loss of vision in one eye. Because the circulation to the entire retina is disrupted, the vision loss is profound and encompasses the entire field of vision. In contrast, a branch retinal artery occlusion only leads to loss of vision in a part of the field of vision. This is because only part of the retinal circulation in compromised. Similar to a central retinal artery occlusion, a branch retinal artery occlusion is also typically sudden and painless.
Evaluation
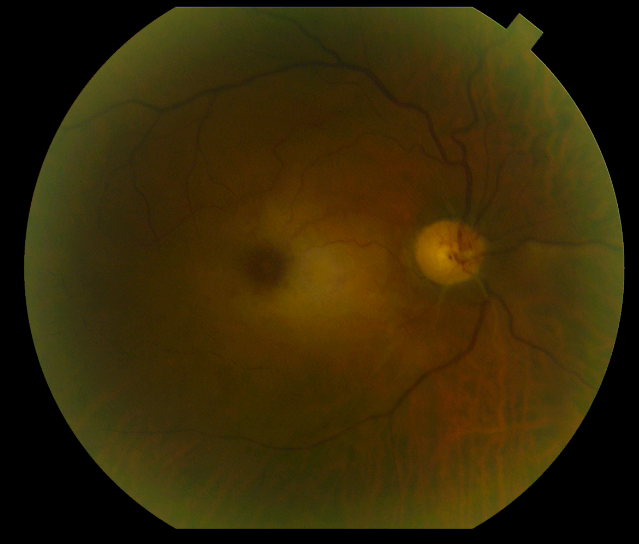
Retinal arterial occlusions can usually be diagnosed simply by examining the retina. Often, the retina is whitened in the area of the occlusion due to the lack of blood flow. Most arterial occlusions occur in patients with diseases such as high blood pressure or diabetes. On occasion, fragments of cholesterol or blood clots can be cause of the occlusion. Therefore, the treating physician will usually order tests looking for the source of these deposits in the carotid arteries or the heart. Another important cause of central retinal artery occlusions is a condition known as temporal arteritis. Temporal arteritis is an inflammatory disorder that can also produce fever, pain, or weight loss. Blood tests are ordered if temporal arteritis is suspected. Figure 1. Whitening of the retina due to a central retinal artery occlusionTreatment
Unfortunately, there is no proven, reliable treatment for retinal arterial occlusions at this time. Various methods including hyperbaric oxygen, ocular massage, and anterior chamber paracentesis may or may not be effective if the occlusion is treated right away. However, if the occlusion is due to temporal arteritis, treatment with corticosteroids is effective at preventing loss of vision in the other eye. An unwanted, late complication of retinal arterial occlusions is neovascularization. Neovascularization refers to the growth of new, abnormal blood vessels in different parts of the eye that can result in bleeding, detachment of the retina, or glaucoma. Neovascularization is treated with laser or injections of anti-neovascular medications into the eye.
Retinal venous occlusions
After blood has passed into the eye through the retinal arteries, it leaves through the retinal veins. Blood travels first through the smaller, branch retinal veins and then enters the central retinal vein.
Symptoms
A central retinal vein occlusion usually causes sudden, painless vision loss in one eye. Unlike a central retinal artery occlusion, which causes profound vision loss, the visual deficit in a central retinal vein occlusion can range from mild to severe. More severe occlusions cause more severe deprivation of vital oxygen to retinal tissue. In addition, a central retinal occlusion can result in macular edema, swelling of the retina that also leads to blurred vision. A branch retinal vein occlusion usually leads to blurring of vision in only part of one eye. Like central retinal vein occlusions, branch retinal vein occlusions can vary in severity, but often result in macular edema as well.
Evaluation
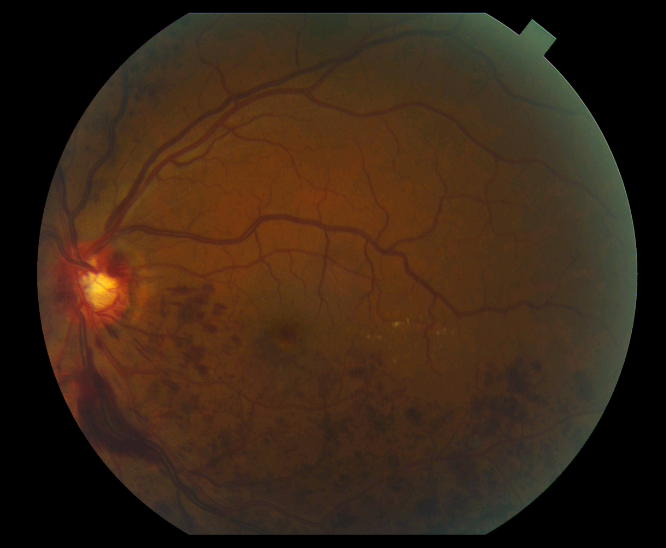
Retinal venous occlusions are also diagnosed by examining the retina. The blocked vein will appear dilated and engorged. In addition, the area of the retina served by that vein will contain hemorrhages or become swollen. To assess the amount of oxygen deprivation to the retina, a specialist will often recommend a fluorescein angiogram. The angiogram involves the injection of a yellow dye known as fluorescein intravenously. Subsequent photos allow visualization of the abnormal blood flow within the retina. In addition, optical coherence tomography is often performed to determine the amount of swelling within the retina. Figure 2. A retinal vein occlusion with hemorrhages seen as the red spots in the bottom half of the image.Treatment
Treatment of retinal venous occlusions is largely aimed at decreasing swelling in the macula in hopes of improving vision. Currently, the most effective treatments involve injections of medication into the eye. FDA approved medications such as Lucentis and Eylea, that target abnormal levels of growth factors in the eye, can result in significant gains in vision in approximately two thirds of patients with branch retinal vein occlusions and half of patients with central vein occlusions. In addition, injectable steroid medications such as Ozurdex can also be effective, with approximately one third of patients having a significant visual gain. Laser can also be used to treat macular edema due to branch retinal vein occlusions. Keep in mind that these treatments likely need to be repeated on a routine basis or used in combination to achieve maximum benefits. If neovascularization occurs, it is treated as previously described in the section about retinal arterial occlusions.
In conclusion, occlusions of either retinal arteries or veins can cause significant visual impairment. Prompt evaluation and ongoing treatment with a retinal specialist can often improve and maintain vision.
Three million people in the U.S. age 40 and older have low vision. According to 2010 research by the National Eye Institute, the number of Americans with low vision will continue to grow dramatically, from 2.9 million in 2010, to 5 million in 2030, to 8.9 million in 2050, as our population ages. In response, The Hadley School for the Blind, the largest provider of distance education for people who are blind or visually impaired worldwide, has launched a series of 10 free audio recordings designed to help those living with low vision maintain their independence. Available through the newLow Vision Focus @ Hadley program the recordings share practical ways to address daily living skills made difficult by vision loss.
Low-Vision Audio Recordings
The recordings are available on CD, NLS (National Library Service) cartridge and as free mp3 audio downloads from the Low Vision Focus @ Hadley (LVF) website at www.lowvisionfocus.org. Individuals are required to register online to receive access to the free audio recordings or they should call 1-855-830-5355 for the CDs or NLS cartridges. Each recording is approximately 30 minutes long and covers a different aspect of living independently with low vision. This series helps people move forward using step-by-step tips and techniques, along with information and resources to help maximize the vision they have.
Following are the 10 audio lesson topics and a sample tip from each:
Making the Kitchen User Friendly
It’s a good idea to have two different cutting boards – a light colored one and another that’s darker. This will allow you to choose a background color that contrasts with the color of the food you’re working with. So, slice white onion or mozzarella cheese on the dark surface, and carrots or green peppers on the light colored board.
Low Vision Cooking
When putting a pan on a burner, make it a habit to move the panhandle over the counter. It’s also a good idea to point it in a consistent direction.
Doing Simple Kitchen Tasks
When you’re cooking with spices, don’t add spices by shaking them over the mixed ingredients, because once you add too much, they can’t be removed. Instead, shake spices into your palm and pinch the amount that you want. You can always add more.
Basic Tactile Marking
When marking a microwave keypad with tactile dots, put one dot on each number – but add an extra dot on the number five. Since the five button is in the middle, the double dot will let you identify it, so you can use it to figure out where the other numbers are around it.
Simple Home Modifications
The direction that the light is coming from is just as important as the source. A lamp with a gooseneck or an adjustable swing arm will help you to position it right where you need the light. Remember, whatever you use, make sure it’s completely shaded, so no light is directed in your eyes making it difficult to see the object.
Getting Around the House
Every place in your home where sound can be heard is a great landmark for the room. Constant sounds like a ticking clock are a great way to tell where you are. Other less dependable sounds like the traffic on the street can tell you where the windows are, your neighbor’s television can let you know where the living room is, and the intermittent motor hum of your refrigerator can always point you towards your kitchen.
Looking Your Best
To mark your shampoo and conditioner, think about it this way: when you’re washing your hair, you use the shampoo first, and the conditioner second. To mark them, just put one rubber band around the shampoo, and then two rubber bands around the conditioner. It’s a simple concept – the container used first gets one mark, and the second gets two.
Keeping Prescriptions in Order
Open your pill bottles over a tray or baking sheet lined with dark colored felt. If you drop a pill, it won’t bounce on the floor and it will be easier to see.
Going Out for a Meal
When reaching for glassware, approach the glass from above, bringing your hand down to the rim, and then to the bottom to pick it up. Putting it down in a consistent place on the table will help you find it more easily.
Going Out with a Friend
A sighted guide is someone who has enough vision to help you get from one place to another safely. You will hold onto their upper arm with your hand so both of you maintain physical contact as you walk. When you’re approaching obstacles or changes in your path like doorways, stairs, or sidewalk curbs, it’s the sighted guide’s job to give you verbal and physical information to keep you aware of the surroundings.
While the LVF is geared toward older adults, the program is open to any individual who is experiencing sight loss or caring for someone who may be losing his or her vision. Adult children of seniors living with low vision are encouraged to take advantage of the online resources to assist their parents. Caregivers and professionals, especially those working with low vision support groups in local communities, are also encouraged to utilize the resources available through the LVF website.
In addition to downloadable recordings, the Web site offers links to free low vision webinars, Hadley distance education courses that are relevant to those with low vision, tips and resource lists. In the future, Hadley will provide free, “quick tip” videos through the Web site that complement the audio recordings as well as new monthly webinars.
“We are so excited to offer Low Vision Focus @ Hadley and enable this growing population to retain their independence and live with confidence,” says VP of Education and Training and head of Low Vision Focus @ Hadley, Doug Anzlovar.


 Crab Toast with Carrot and Scallion – Forget your traditional bruschetta, wow your guests with the appetizer.
Crab Toast with Carrot and Scallion – Forget your traditional bruschetta, wow your guests with the appetizer. Potato-Carrot Latkes with Lemon-Raisin Topping – Seems perfect with Hanukkah just around the corner.
Potato-Carrot Latkes with Lemon-Raisin Topping – Seems perfect with Hanukkah just around the corner. Roasted Carrot, Squash and Sweet Potato Soup – This is a more traditional carrot recipe, it is not that hard to find a carrot soup, but this one also has squash and sweet potatoes which are also eye healthy!
Roasted Carrot, Squash and Sweet Potato Soup – This is a more traditional carrot recipe, it is not that hard to find a carrot soup, but this one also has squash and sweet potatoes which are also eye healthy! Carrot Farfalle Pasta with Lemon and Herbs – Not only are carrots good for flavor, but they add a nice color to this pasta that could be the base for any number of pasta dishes.
Carrot Farfalle Pasta with Lemon and Herbs – Not only are carrots good for flavor, but they add a nice color to this pasta that could be the base for any number of pasta dishes. Carrot Ginger Layer Cake with Orange Cream Cheese Frosting – Most carrot cakes have no frosting or a traditional cream cheese frosting. The idea of an orange frosting makes this cake special.
Carrot Ginger Layer Cake with Orange Cream Cheese Frosting – Most carrot cakes have no frosting or a traditional cream cheese frosting. The idea of an orange frosting makes this cake special. Carrot, Ginger, and Lime Juice – Refreshing and healthy.
Carrot, Ginger, and Lime Juice – Refreshing and healthy. Susan DeRemer, CFRE
Susan DeRemer, CFRE